ARNFINN HELLEVE (1), MAJA WEEMES GRØTTING (1, 2), DINA HEIDER HOV (2), TARA KELLY DOLGNER (3), ELISABETH KVAAVIK (2)
(1) Centre for Evaluation of Public Health Measures, Norwegian Institute of Public Health, (2) Department for Alcohol, Tobacco and Drugs, Norwegian Institute of Public Health, (3) Department for Research Administrative Support, Norwegian Institute of Public Health
Background
In collaboration with six hospitals, the Norwegian Institute of Public Health conducted a study of the effectiveness of offering a smoking cessation program to cancer patients in treatment. The program consisted of at least four individual counselling sessions based on Motivational Interviewing and offered cost-free nicotine replacement therapy to cancer patients who were entering treatment. The Norwegian Cancer Society funded the study.
In addition, we assessed implementation of the program and present the findings regarding smoking status among the referred patients, as well as tobacco use habits and demographic data for the study participants at the start of the study.
Methods
The study period took place from September 2017 until March 2020 and included an intervention group and a control group. The intervention group received structured smoking cessation guidance based on Motivational Interviewing, combined with offering cost-free smoking cessation medication (nicotine replacement therapy) while the control group received the individual hospital’s standard smoking cessation program or measures. Cancer patients age 18 years and older who smoked and were referred to cancer treatment at one of six participating hospitals were invited to participate. Only cancer patients with an estimated survival of at least 12 months, not suffering dementia or other mental illness affecting the capacity to give informed consent, were invited. Due to practical and ethical considerations, we chose a design where both the control and intervention group participants were recruited by the same hospital department, but during two different time periods. The control group’s recruitment and baseline questionnaire were completed one month before recruitment to the intervention group began.
Participants were invited to answer a questionnaire at baseline and to answer a follow-up questionnaire after six months. The recruiting period lasted from 1. September 2017 to 1. March 2019 for the control group and from 1. March 2019 to 1. March 2020 for the intervention group. The participants in the intervention group received information and an offer to participate in the structured smoking cessation program, while the control group participants were offered the individual hospital’s standard smoking cessation program or measures. In the study we included only participants with both baseline and follow-up data in the two study groups (n=201).
After completing the follow-up questionnaire in the intervention group, smoking behaviour among participants in the two groups was compared. In addition, a process evaluation was conducted, where the purpose was to examine how the study and the program were implemented at the participating hospitals.
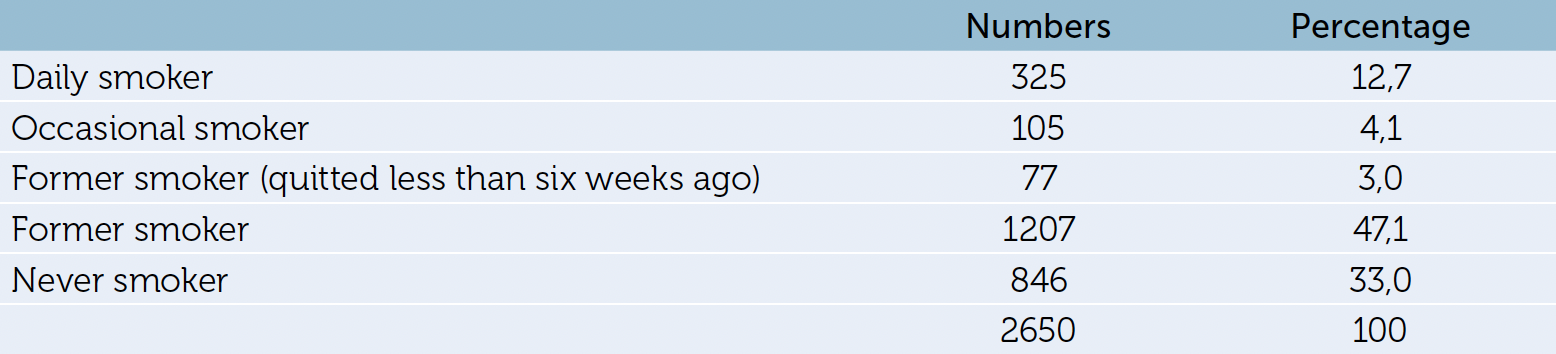
Table 1: Self-reported smoking behaviors among all patients referred to the study hospitals during the study period (n=2560).
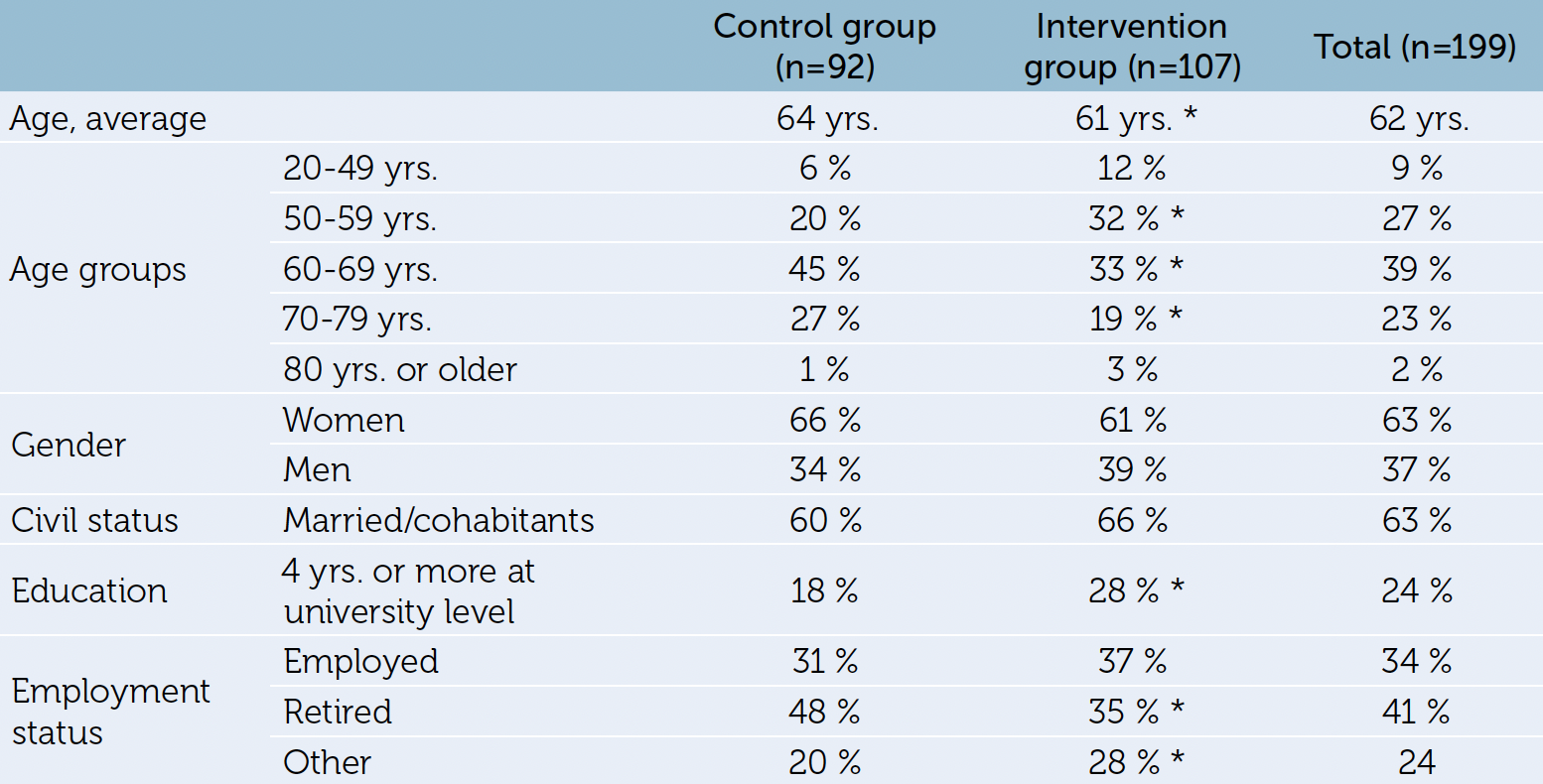
Table 2: Socio-demographics of the study participants in the effectiveness study (participants with baseline and follow-up measurements) (n=199). *) p<0,05, t-test between intervention and control group

Table 3: Smoking status at baseline and follow-up (after six months) (n=201).
1) “Former smoker” is the term used for participants who quit smoking less than six weeks before study start
Results
The average age of the participants overall was 62 years, while the average age was significantly higher in the control group than in the intervention group: 64 and 61 years, respectively1. There were more female participants (63 %) than male. The intervention group had a larger proportion of participants with a higher education and a smaller proportion of retired participants compared to the control group. There was a slightly higher dropout rate in the intervention group than in the control group (54 % and 51 %, respectively).
At the 6-month follow-up, we found a statistically significant decrease in the proportion who smoked (daily and occasional smoking combined) in both study groups. Nevertheless, there was a significantly larger decrease in smoking among the patients in the intervention group compared to patients in the control group. The difference was 12 percentage points (p-value 0.043). After adjusting for gender, age, education, labour market participation and cohabitation, the effect increased by around two percentage points, i.e. a 14-percentage point difference for the decrease in smoking.
Findings from the process evaluation indicated that there may be organizational challenges at the hospitals related to the identification of patients who smoke and the capacity to offer guidance when patients show up for treatment. There were also some variations between individuals and professions in their ownership to the provision of the smoking cessation program. The smoking cessation counsellors’ impression was that patients appreciated that the counselling approach was friendly and not judgemental. Some of the counselling sessions were conducted by telephone, and the number of counselling sessions that the participants received varied.
Discussion
The positive study results in the study must be seen in the light of several methodological challenges. These challenges may affect the validity of the results. First, participation in the study was unfortunately lower than expected, with about one-fifth of the planned participation, based on strength calculations. This has an impact on the accuracy of the results and the interpretation of these. Another challenge is the high drop-out rate of participants between baseline and follow-up and the fact that the drop-out rate differed between the groups. This drop-out may be problematic if those who have responded to the follow-up are those who have benefited the most from the smoking cessation intervention.
Another challenge is related to the actual design of the study. Ideally, the study should have been conducted as a randomized controlled trial by randomizing patients to the intervention group or the control group at the same hospital or between hospitals. However, this was considered as unethical as well as challenging for the participating hospitals, and therefore the study was conducted with a serial design. This can introduce two types of problems. First the fact that participants in the two groups participated during different periods. In the course between these time periods, the involved health personnel’s attitudes towards smoking might have changed and possible new smoking prevention measures implemented during the project period may have affected the groups differently. Second, participants were not randomized to a group, but were invited to either the control group or the intervention group.
Regarding the smoking cessation program that the patients were offered, the feedback from the smoking cessation counsellors was that the guidance based on Motivational Interview had worked well. The initial plan was that each patient would receive at least four hours of counselling, but the results indicate that there have been considerable variations in number of counselling sessions the patients received.
Conclusion
This study demonstrated a positive effect of offering a structured smoking cessation program to cancer patients under treatment. The program of individual counselling sessions based on Motivational Interviewing and offering cost-free nicotine replacement therapy for those who wanted it was compared to the pre-existing individual hospital’s standard smoking cessation program or measures. The results may indicate that around 10 % more cancer patients will stop smoking if they receive an offer like this: of the patients who were registered at the 6-month follow-up, approximately 30 % of the control group had quit smoking, whereas about 40 % of the intervention group had quit smoking.
The registration of smoking habits among patients who came for treatment showed that around 20 % were smokers or had only recently (< 6 weeks) quitted smoking. This provides an indication of how many patients can benefit from such an offer. A smoking cessation program for cancer patients who are entering treatment should become an integrated part of oncological care and should be rooted in the entire organization.
1 We registered smoking behaviour among 2.560 cancer patients referred to five of the study hospitals during the recruitment period of the study. Approximately 17 % of the referred cancer patients smoked daily or occasionally. In addition, 3 % had only very recently quit smoking and were therefore considered as smokers and eligible as study participants. The proportion of smokers among referred cancer patients is on par with the proportion of smokers in the population in the same age groups (55 years and older).