Karin Lindberg. MD, PhD, Karolinska Institutet, HHLH-sektionen, Tema Cancer, Karolinska Universitetssjukhuset Solna, Stockholm
Stereotactic body radiation therapy (SBRT) has been a major leap in the treatment of cancer. SBRT is a radiation therapy technique in which a few high-dose fractions are delivered to a well-defined target in the body, rendering extremely high biological doses. In metastasized patients, SBRT is mainly used in the oligometastatic setting – a condition of early metastatic disease with a limited number of metastases (usually ≤5) in a limited number of organ systems (usually ≤3) (1, 2). The theory here is that eradication of macroscopic tumors using SBRT, while controlling the microscopic disease with systemic therapy, may render prolonged survival (2), which has been supported by recently published clinical data (3). In the metastatic setting, SBRT may now be actively integrated either as up-front therapy in the oligometastatic setting or as an adjunctive to systemic therapy to ablate drug resistant tumor cell clones. This article will focus on the outcome of SBRT of metastases from colorectal cancer and the future integration of SBRT in the metastatic treatment.
Stereotactic body radiation therapy – overview of the technique
In the mid 1990-ties, stereotactic body radiation therapy (SBRT) was developed at Karolinska University Hospital in Stockholm Sweden. This non-invasive radiation therapy technique offers high precision radiotherapy in which a few fractions (normally 3-8) with high doses (7-17Gy) are delivered to a well defined intra-corporal target with small margins (5-10 mm) of normal tissue. The treatment is delivered in 1-2 weeks, which is convenient for the patient. Generally, the dose is prescribed to the ⁓67-80% isodose line encompassing the planning target volume (PTV), resulting in central doses of 125-150% of the prescription doses. Originally, the tumor position was verified in a 3-D-coordinate system using the stereotactic body frame. Further technical developments now allow for correction of the tumor position using daily on-line image guidance and tailoring of the dose distribution with volumetric modulated arc therapy (VMAT), which may be advantageous if the target is close to a radiation sensitive risk organ, as well as gating and tracking of the tumor during treatment. Today, SBRT is used in the everyday clinic to treat tumor lesions in various organ sites such as the lungs, the liver, the lymph nodes, the adrenals and the bones, achieving high rates of local control (>80%).
SBRT of lung lesions from colorectal cancer
SBRT has mainly been evaluated for patients with peripherally located early stage non-small cell lung cancer (NSCLC) suffering from pulmonary and cardiac co-morbidities rendering them medically inoperable. Increasingly also peripherally located pulmonary metastases from various primaries are treated. Both these patient groups show excellent local control of >90% and acceptable side effects despite the generally frail baseline medical status of the patients (4, 5). The most commonly reported side effects are low-grade cough, dyspnea, fatigue, pleural effusion, skin reaction and regional fibrosis in the high-dose area. Metastases from colorectal cancer (CRC) comprise one of the most common histologies in this setting and interestingly may inhabit an increased radioresistance, possibly requiring higher doses to achieve local control as compared to tumours with other histological origin. This issue was addressed in a restropective study (6) comparing SBRT of CRC-metastases versus non-CRC-metastases versus primary NSCLC. The authors here noted a significant difference with inferior local control for CRC-metastases as compared to non-CRC-metastases (2-year-local control 73% vs 94%) with tumor origin being the only significant factor in multivariate analysis. This however, was a Japanese study using a homogenous dose of 10Gy x 5 (corresponding to BEDα/β10Gy, 100Gy) and the different subgroups were small. A possible mechanism behind this radioresistance with CRC-histology might be an increased ratio of hypoxic cells. There are also implications that clinical and treatment related factors such as pre-treatment chemotherapy may have negative impact on local control (7). Takeda and colleagues concluded that dose escalation might overcome this resistance and as seen from later published material including a meta-analysis from 2018 of more than 600 patients with pulmonary CRC-metastases, this seems to hold true (8). However, no optimal dose for SBRT of CRC metastases have been set, but many centers use higher fraction-doses for CRC-metastases as compared to those used for metastases from other primaries.
Peripherally located lung lesions may thus be treated with excellent outcome. Centrally located lesions on the other hand, often pose a challenge and the role of SBRT in this situation is currently unclear. Early attempts with SBRT using the same high dose per fraction as those used for peripherally located lesions, caused excessive toxicity and treatment related death. However, some later presented reports support the use of SBRT for central lesions when using modified fractionation schedules whereas other reports still raise a warning finger. The latter especially concerns ultracentrally located lesions with tumors abutting the proximal bronchial tree or the planning target volume (PTV) overlapping a main bronchus; situations where high grade toxicity has been observed (9, 10). Currently there is no consensus on how to treat these lesions with SBRT and dose constraints to relevant organs at risk, remain uncertain. Hopefully the results from the Nordic HILUS-trial – a prospective phase II study of SBRT of extremely centrally located lung lesions conducted within the Nordic SBRT study group – will enlighten this issue (final results in the near future). Apically located lung lesions may also be challenging to treat, considering the proximity to the brachial plexus. Here there is a delicate balance between keeping the dose to the target, to avoid tumor recurrence, and at the same time not exceed the dose tolerance of the brachial plexus, which may result in debilitating radiation induced brachial plexopathy.
SBRT of liver metastases from colorectal cancer
Long-term results from surgical metastasectomy of liver metastases from CRC cancer are indeed good (⁓25% at 10 years). However, 40-90% of the patients are inoperable due to the patient´s medical status, the extent of the disease, comorbidities or technical considerations. Generally, SBRT of liver tumors is a successful treatment with local control rates of 70-92% and 91% at 2 and 4 years respectively (all histologies). The most commonly encountered side effects include fatigue, pain, transient elevated liver enzymes, nausea, diarrhea and skin reaction, presenting in low grades. Grade 3 and higher toxicity occurs in a frequency of ≤2% as concluded from prospective studies (11, 12). However, metastases from CRC may also here possess an increased radioresistance. A study published in 2017 on liver metastases from CRC, found a statistically significant difference in local control between three dose levels (≤80Gy, 100-112 Gy, 132-180Gy (BEDα/β10Gy)) with a 2-year-local control rate of 89% for the highest dose level group (13). Local control rate at 2 years post SBRT of liver metastases from CRC ranges between 73-91% based on materials using at least a prescription dose of 106Gy (BEDα/β10Gy) (12-14) and 2-year-overall survival rate ranges between 56-75% (12, 14, 15). A pooled study from last year based on 18 studies with 656 patients included, showed a progression free survival of 11.5 months, but a somewhat inferior local control of 67% and 59% at 1 and 2 years respectively. A possible explanation might be that a number of studies included in the analysis had a wide range of prescription doses, some with the inferior limit as low as 31 Gy (BEDα/β10Gy) (15). In metastases from CRC a site dependent radiosensitivity, with liver metastases requiring higher doses for local control (compared to lung metastases) has also been suggested (7, 16). Possible explanations might be the histological differences between the two organs or may reflect tumor/technical treatment related differences (challenges in target volume delineation, motion management, increased radioresistance due to prior chemotherapy for example) (7).
How does SBRT effect the disease outcome?
Metastases from CRC at various tumor locations in the body may thus be successfully treated with SBRT, but how does SBRT impact the overall treatment effect in terms of time to progression and survival? Survival post SBRT of pulmonary metastases have been reported up to 77% at 2 years and 39% at 5 years (17, 18). In an interesting study, comparing surgery and SBRT of pulmonary metastases (retrospective analysis of 110 consecutively treated patients undergoing surgery or SBRT for pulmonary metastases from any histological origin) the 3- and 5-year-overall survival rates were comparable between the two groups (60/62% and 41/49% respectively) (19). As mentioned above, 2-year-overall survival (56-75%) post SBRT of liver metastases have also been favorable, bearing in mind that patients considered for SBRT possibly may have had non-favorable base-line characteristics as compared to patients undergoing surgery for the same indication. Reported pre-treatment related factors affecting PFS and OS varies greatly. In SBRT of lung metastases (from CRC) ECOG 0-1, female gender, > 2-year-interval from cancer diagnosis to metastatic spread and no extra lung sites were associated with better PFS, whereas prior treatment with chemotherapy with or without local treatment was associated with worse PFS. In analyses of SBRT of metastases at any site in the body (from CRC), lung metastases only, left-sided primary tumor, KRAS wild type, complete remission or partial response to 1st line chemotherapy, 1-3 treated lesions and prescription doses >100 Gy (BEDα/β10Gy) have been associated with better PFS. The impact of local control of the SBRT-treated target on survival has been uncertain but a study from this year (388 patients with 500 pulmonary and/or hepatic metastases from CRC) suggests that local control improves long-term survival, if the projected OS is longer than 12 months (7).
SBRT in the oligometastatic setting
Retrospective analyses have reported long-term survival of patients with oligometastases undergoing SBRT, but it is difficult to know whether this is based on favorable tumor biology and patient selection or a result of the treatment itself. Questions that are central to this issue include: How do we best measure the efficacy of SBRT (OS, PFS, local control)? What do the results show – effect of a treatment or tumor biology? How do we pick out the patients suitable for local ablative therapy and what is the optimal integration of SBRT with systemic treatment? Figure I shows a few examples of how SBRT may be used for three different patients with metastatic CRC, heightening the complexity in deciding the optimal point of time and indication for SBRT in relation to other treatments. At Karolinska, based on previously treated patients, we have constructed a prediction model for SBRT of CRC metastases to be used as a decision-support-tool for whom to treat (validation of the model is currently planned). The model is planned to be web-based and directly usable in the everyday clinic.
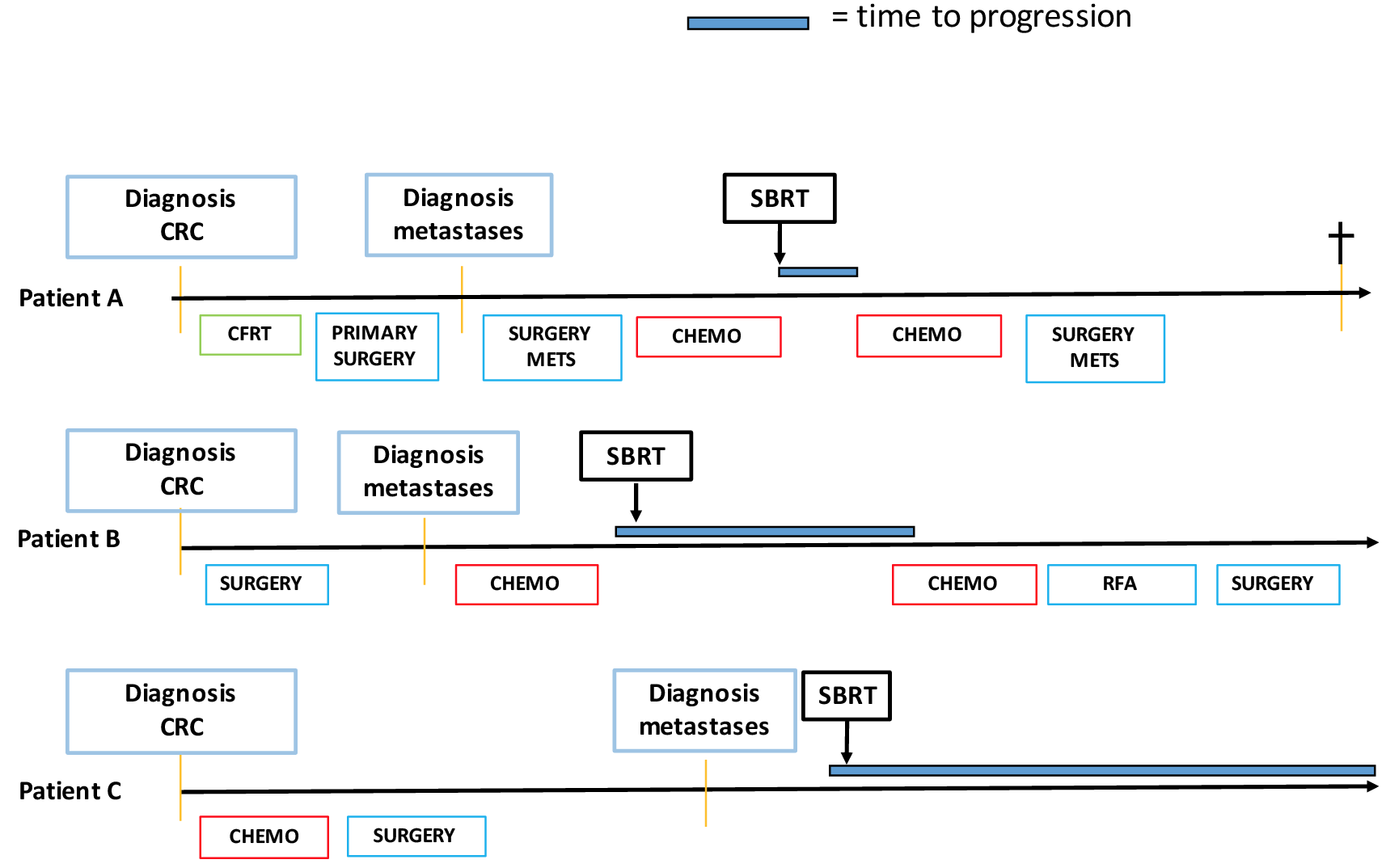
Figure I: Examples of three patients treated with SBRT for CRC metastases with different indications: as treatment beyond progression on systemic therapy (patient A), as consolidation therapy (patient B) and as upfront treatment for oligometastases (patient C).
Local ablative therapies for oligometastases have lately also been addressed prospectively. In non-small cell lung cancer (NSCLC), a few small randomized trials have shown promising results with significant improvement of survival after ablative treatment to metastatic lesions in comparison to standard of care. Recently the SABR-COMET-trail (a randomized multicenter phase II trial comparing medical standard of care treatment alone with medical standard-of-care and SBRT to all metastatic lesions) (3) showed extremely encouraging results, reporting median PFS improving from 6 to 12 months (HR 0.47; 95%CI 0.30-0.76, p=0.0012) and median OS improving from 28 to 41 months (HR 0.57, 95% CI 0.3-1.10, p=0.09) for the patients randomized to the combination arm (mixed diagnoses, 18% with CRC). These results are truly encouraging especially in light of the parallel rapid development of new systemic treatments and opens up for a paradigm shift in the treatment of metastatic cancer. Patients with metastases may render exceptional responses and return to their ordinary life, living with a chronic disease.
Today, SBRT is a valid local treatment option for patients with metastases from CRC. The great challenge here is to pick out the patients benefitting from the treatment and to tailor a personalized combination of systemic and local ablative treatments aiming for prolonged time to progression with maintained good quality of life and ultimately increased survival.

CT-bilder med post-SBRT lungeforandringer
«The great challenge is to pick out the patients benefitting from the -treatment»
References
- Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. 1995;13(1):8-10.
- Rusthoven CG, Yeh N, Gaspar LE. Radiation Therapy for Oligometastatic Non-Small Cell Lung Cancer: Theory and Practice. Cancer J. 2015;21(5):404-12.
- Palma DA, Olson R, Harrow S, Gaede S, Louie AV, Haasbeek C, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial. Lancet. 2019;393(10185):2051-8.
- Rusthoven KE, Kavanagh BD, Burri SH, Chen C, Cardenes H, Chidel MA, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for lung metastases. J Clin Oncol. 2009;27(10):1579-84.
- Baumann P, Nyman J, Hoyer M, Wennberg B, Gagliardi G, Lax I, et al. Outcome in a prospective phase II trial of medically inoperable stage I non-small-cell lung cancer patients treated with stereotactic body radiotherapy. J Clin Oncol. 2009;27(20):3290-6.
- Takeda A, Kunieda E, Ohashi T, Aoki Y, Koike N, Takeda T. Stereotactic body radiotherapy (SBRT) for oligometastatic lung tumors from colorectal cancer and other primary cancers in comparison with primary lung cancer. Radiother Oncol. 2011;101(2):255-9.
- Klement RJ, Abbasi-Senger N, Adebahr S, Alheid H, Allgaeuer M, Becker G, et al. The impact of local control on overall survival after stereotactic body radiotherapy for liver and lung metastases from colorectal cancer: a combined analysis of 388 patients with 500 metastases. BMC Cancer. 2019;19(1):173.
- Jingu K, Matsushita H, Yamamoto T, Umezawa R, Ishikawa Y, Takahashi N, et al. Stereotactic Radiotherapy for Pulmonary Oligometastases From Colorectal Cancer: A Systematic Review and Meta-Analysis. Technol Cancer Res Treat. 2018;17:1533033818794936.
- Tekatli H, Haasbeek N, Dahele M, De Haan P, Verbakel W, Bongers E, et al. Outcomes of Hypofractionated High-Dose Radiotherapy in Poor-Risk Patients with «Ultracentral» Non-Small Cell Lung Cancer. J Thorac Oncol. 2016;11(7):1081-9.
- Haseltine JM, Rimner A, Gelblum DY, Modh A, Rosenzweig KE, Jackson A, et al. Fatal complications after stereotactic body radiation therapy for central lung tumors abutting the proximal bronchial tree. Pract Radiat Oncol. 2016;6(2):e27-33.
- Rusthoven KE, Kavanagh BD, Cardenes H, Stieber VW, Burri SH, Feigenberg SJ, et al. Multi-institutional phase I/II trial of stereotactic body radiation therapy for liver metastases. J Clin Oncol. 2009;27(10):1572-8.
- Scorsetti M, Comito T, Tozzi A, Navarria P, Fogliata A, Clerici E, et al. Final results of a phase II trial for stereotactic body radiation therapy for patients with inoperable liver metastases from colorectal cancer. J Cancer Res Clin Oncol. 2015;141(3):543-53.
- Joo JH, Park JH, Kim JC, Yu CS, Lim SB, Park IJ, et al. Local Control Outcomes Using Stereotactic Body Radiation Therapy for Liver Metastases From Colorectal Cancer. Int J Radiat Oncol Biol Phys. 2017;99(4):876-83.
- Comito T, Cozzi L, Clerici E, Campisi MC, Liardo RL, Navarria P, et al. Stereotactic Ablative Radiotherapy (SABR) in inoperable oligometastatic disease from colorectal cancer: a safe and effective approach. BMC Cancer. 2014;14:619.
- Petrelli F, Comito T, Barni S, Pancera G, Scorsetti M, Ghidini A, et al. Stereotactic body radiotherapy for colorectal cancer liver metastases: A systematic review. Radiother Oncol. 2018;129(3):427-34.
- Ahmed KA, Fulp WJ, Berglund AE, Hoffe SE, Dilling TJ, Eschrich SA, et al. Differences Between Colon Cancer Primaries and Metastases Using a Molecular Assay for Tumor Radiation Sensitivity Suggest Implications for Potential Oligometastatic SBRT Patient Selection. Int J Radiat Oncol Biol Phys. 2015;92(4):837-42.
- Filippi AR, Badellino S, Ceccarelli M, Guarneri A, Franco P, Monagheddu C, et al. Stereotactic ablative radiation therapy as first local therapy for lung oligometastases from colorectal cancer: a single-institution cohort study. Int J Radiat Oncol Biol Phys. 2015;91(3):524-9.
- Mihai A, Mu Y, Armstrong J, Dunne M, Beriwal S, Rock L, et al. Patients with colorectal lung oligometastases (L-OMD) treated by dose adapted SABR at diagnosis of oligometastatic disease have better outcomes than patients previously treated for their metastatic disease. J Radiosurg SBRT. 2017;5(1):43-53.
- Widder J, Klinkenberg TJ, Ubbels JF, Wiegman EM, Groen HJ, Langendijk JA. Pulmonary oligometastases: metastasectomy or stereotactic ablative radiotherapy? Radiother Oncol. 2013;107(3):409-13.