
Dr. Vitaly Smelov

Trols E. Bjerklund Johansen
Av: Prof. Truls E. Bjerklund Johansen, Dept of Urology, Oslo University Hospital
Dr. Vitaly Smelov, IARC WHO Prevention and Implementation Group, Lyon, France
Co-authors: Kurt Naber (Germany) and Florian Wagenlehner (Germany)
Urine microbiome: A new paradigm in urogenital infections and diseases
A paradigm shift
Until recently the generally accepted paradigm implied that urine of healthy people is sterile. In case of urinary tract infection (UTI) a significant bacteriuria is estimated by the number of colonies of known uropathogens (Figure 1).
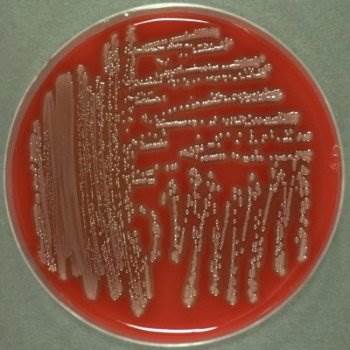
Figure 1. Outcome of culture. Colonyforming units of E.coli in a Petri dish diagnosed by inspection
In the meantime numerous studies have shown that many different microorganisms might be detected in the urine of practically all healthy people, if cultured on specially enriched media (1,2). Further, the development of metagenomic sequencing technologies (MGS) and the introduction of bioinformatics enabled us to analyze complete genomes of microorganisms and brought us into the omics era (Figure 2) (3). The word microbiome was introduced to describe the “characteristic microbial community occupying a reasonably well defined habitat which has distinct physico-chemical properties. The term not only refers to the micro-organisms involved but also encompasses their theatres of activity” (4).
Man`s urine meets the criteria for being a habitat with its own microbiome. We have learned that the urogenital tract in healthy people might harbor genomes from more than a hundred different micro-organisms. This information challenges our reference points and the principles for classification of diseases of the urogenital tract (5).
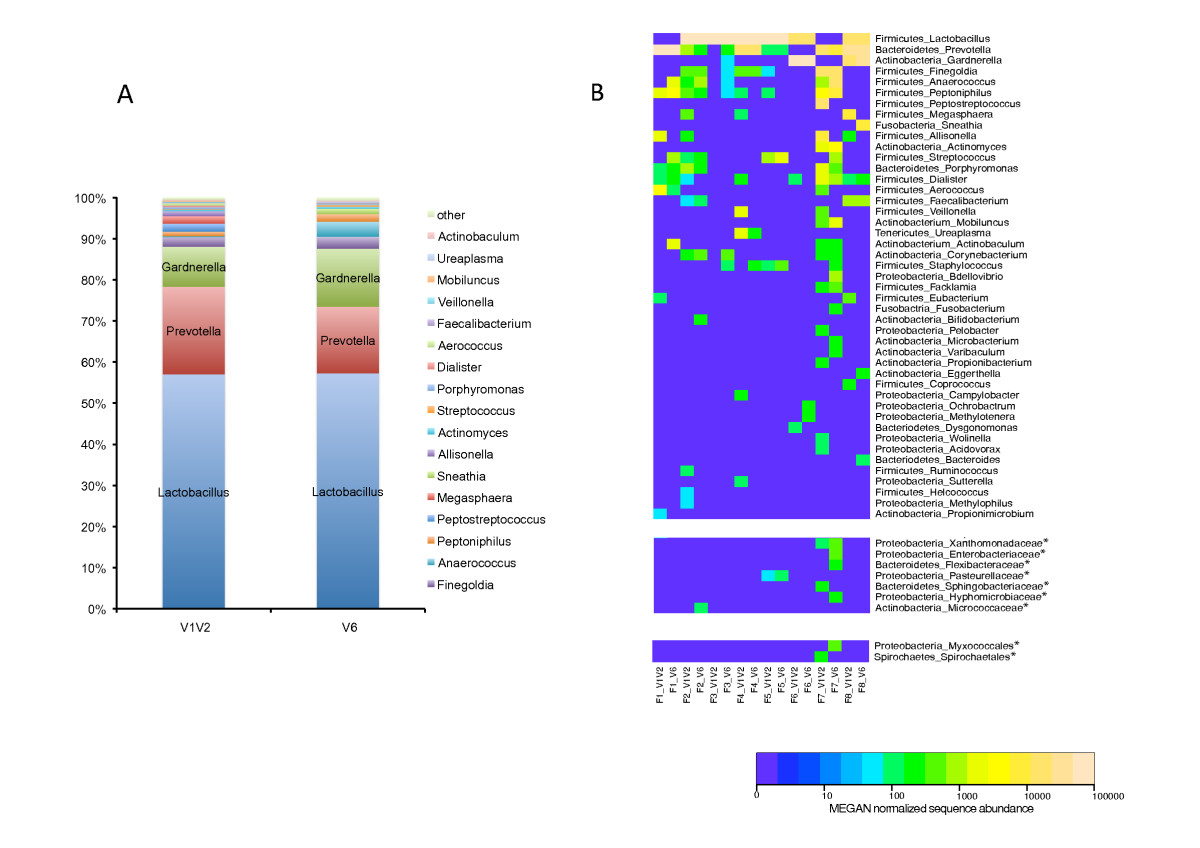
Figure 2.
Outcome of 16S rDNA sequencing. Bacterial genera detected in healthy female urine. Reprinted from (3)
A: Comparison of healthy female urine bacterial genera abundance determined by sequencing 2 different hypervariable 16S rDNA regions, V1V2 and V6. Relative abundance of 18 major bacterial genera found in the sequence pool of eight different urine samples are shown for the two 16S rDNA regions. Groups denoted ”other” represent minor groups classified. Y-axis represents relative abundance. B: Heat map showing the relative abundance of bacterial genera across urine samples of eight healthy females. Genera denoted as phylum-genus, samples denoted as samplenumber_V1V2 or V6. Taxa marked with asterisk (*) could not be assigned to any genera, and are shown at the lowest common taxon: family and order. Color intensity of the heat map is directly proportional to log 10 scale of the abundance normalized sequence data as done by MEGAN.
Disease classification
Symptomatic UTIs are defined as a host reaction by way of symptoms, findings of white cells or other immune reaction mediators as well as evidence for the presence of a causative pathogen. By early consensus, the significant number of pathogens was set at 105 colony forming units per milliliter (6). This number is modified by the clinical situation, the sampling technique and the identity of the suspected pathogen, for example a CFU of 102 is considered significant when urine is sampled by suprapubic puncture (7,8). In general, the critical number of CFUs has been lowered with time and for tuberculosis, we use to say that detection of a single bacillus is enough to diagnose the disease. Importantly, the lower the colony counts, the higher the likelihood of contamination.
Some urological diseases have been defined by the presence of micro-organisms (urethritis, prostatitis, cystitis, pyelonephritis, sepsis), others by the absence of micro-organisms (overactive neurogenic bladder, female urethral syndrome, bladder pain syndrome/interstitial cystitis and chronic pelvic pain syndrome/ chronic inflammatory prostatitis), and others again by the evidence of a host immune response (white cells in EPS of chronic prostatitis IIIa, Mast cell response in interstitial cystitis). As extended cultures and sequencing studies demonstrated the presence of micro-organisms in healthy people and in diseases where the diagnosis is based on “sterile urine”, we had to acknowledge that the concept of sterile urine was a myth (5).
However, sequencing technologies do not tell if genomes in the urine stem from living or dead micro-organisms and clinicians must keep in mind that antibiotics are only effective against living organisms. From a clinical perspective the term “sterile urine” might therefore be replaced by “being without significant numbers of culturable uropathogens”. Interestingly, the EAU Section of Infections in Urology (ESIU) classification of UTI from 2010 is the only classification that considers treatability by antibiotics as a criterion for severity assessment (9). This classification is therefore in a good position to be developed further depending on new findings about the role of the microbiome in various urological diseases (10).
The host reaction
The symptom language of the lower urinary tract is very much the same in diseases thought to have different etiology and most symptoms can be explained as a host reaction. As metagenomic sequencing reveals that the presence of micro-organisms in the genitourinary tract is very diverse and varies with sex, age and sexual activity, the interplay between the genes of the micro-organisms and the host is becoming more interesting.
From the field of infections we know that the host reaction is precipitated by micro-organisms invading urothelial cells or the blood stream. In patients with symptomatic UTI, there is a strong correlation between urinary IL-8 levels and urinary neutrophil numbers (11). Children prone to develop pyelonephritis have lower expression levels of chemokine receptors (CXCR1) than healthy controls and multiple mutations in the CXCR1 gene have been identified (12).
Mice that are lacking toll like receptor 4 (TLR4) do not develop inflammation and symptoms of UTI if they are challenged with uropathogenic E. coli. Likewise, it has been shown that children with dysfunctional TLR4 due to gene polymorphism are susceptible to develop asymptomatic bacteriuria (ABU) with a low inflammatory response rather than symptomatic infection (13).
Details of the immunological host response provide evidence for a genetic predisposition towards development of UTI and ABU. As this information is being unveiled our scientific focus is moving from identification of single uropathogens in the diagnosis infections to the role of genes from bacteria and viruses in the pathogenesis of urological diseases in general.
Carcinogenesis
We have known since long that there is a relationship between infections and cancer like in Helicobacter pylori and gastric cancer; Epstein-Barr virus and Non-Hodgkin´s and Burkitt`s lymphomas; and Human herpes virus 8 and Kaposi sarcoma. Within the genitourinary tract there is a relation between Schistosoma hematobium and bladder cancer and between Human Papilloma Virus and several urogenital cancers. A relevant clinical experience is that immune deficiency increases the risk of developing both infections and cancer in the genitourinary tract.
There are many similarities between sexually transmitted infections and cancer in terms of invasion, spread through lymphatic vessels to regional lymph nodes and through blood vessels to distant organs. Years of latency and resistance to effective drug treatment are seen in both infections and cancer.
Carcinogenesis may be caused by DNA from microorganisms exploiting the host cellular machinery for transcription and replication thereby interfering with genetic and epigenetic control mechanisms for differentiation and proliferation. These mechanisms are well described for HPV where there is latency of 10-30 years between infection and the manifestation of a malignant tumor and where an effective vaccine is now available (14). Another mechanism which is met with increasing interest in prostate cancer is the effect of chronic inflammation which may cause DNA damage through oxidative stress and reactive oxygen species (15). As for infections, polymorphisms of cytokine genes have been suggested as risk factors for prostate cancer development, and significant associations have been observed between prostate cancer and promoter variants in VEGF, IL8 and IL10 (16).
TLRs with its 10 subtypes have a key role in angiogenesis, neoplasia and inflammatory response. TLRs interplay with DAMP (damage-associated molecular pattern) and PAMP (pathogen-associated molecular pattern) from both tumor and non-tumor micro-environments and TLRs appear to be a commonality in the pathogenesis of infection and cancer (17). Numerous studies are exploring the possibilities of TLR activation to enhance the immune response and TLR inhibition to induce tolerance and decrease cancer-promoting gene activation in different malignant tumors (18). Furthermore, micro-organisms and prostate cancer cells have evolved similar strategies to evade destruction by responding to environmental pressure and both are undergoing selective evolution through genetic change.
The role of genomes of micro-organisms in urinary tract carcinogenesis has become a research era of explosive growth which is triggered by metagenomic sequencing.
Antibiotic treatment
Genomes from lots of bacteria and viruses may now be detected in urine and expressed prostatic secretion in healthy individuals. These genomes most likely stem from bacteria or viruses within the urothelial cells. From studies with enhanced culture techniques, we know that many microorganisms are alive and hence may be killed by antibiotics. It is largely unknown how the different microorganisms interact, but some commensals do prevent uropathogens from dominating the battlefield. A protective effect of commensals is supported by the negative effects of antibiotic treatment of asymptomatic bacteriuria in women (19). This is also the principle behind probiotic treatment with lactobacilli and bladder instillation treatment with apathogenic types of E. coli to prevent recurrences of UTI with uropathogenic E. coli (20).
All bacteria that are exposed to antibiotics may develop resistance, not just the causative pathogens in UTI. There is also a risk that members of the normal human microbiome become extinct for certain periods of time. Recognition of the big diversity of micro-organisms makes it clearer to us that using broad spectrum antibiotics for prophylaxis and treatment is to shoot sparrows with cannons. This is the rationale for recent studies on treatment of UTI with anti-inflammatory drugs only, for phytotherapy and for the development of antibodies against specific types of uropathogens. Moreover, the frequent use of antibiotics has strikingly been associated with an elevated risk of some malignancies (21).
Future research
The concept of a urine microbiome has introduced a new paradigm in our understanding of urogenital infections and urological diseases in general. Our focus is shifting from pathogens to genes and the microbiome in general and numerous questions arise. When do all the different microorganisms enter the urinary tract, when are they alive, what is their interaction with each other and what is their role in the development of infections, stones, cancer, and other urological diseases? What is the effect of antibiotic prophylaxis and antibiotic treatment on the microbiome? A vast new research field is waiting to be explored.
References
- Hilt E, McKinley K, Pearce MM, Rosenfeld AB, Zilliox MJ, Mueller ER, Brubaker L, Gai X, Wolfe AJ, Schreckenberger P: Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol 2014; 52: 871–876.
- Kogan MI, Naboka YL, Ibishev KS, Gudima IA, Naber KG. Human urine is not sterile – shift of paradigm. Urologia Internationalis 2015;94(4):445-52
- Siddiqui H, Nederbragt AJ, Lagesen K, Jeansson SL, Jakobsen KS. Assessing diversity of the female urine microbiota by high throughput sequencing of 16S rDNA amplicons. BMC Microbiol. 2011 (Nov 2);11:244. doi: 10.1186/1471-2180-11-244.
- Lederberg, J; McCray, AT (2001). ”’Ome Sweet ’Omics-a genealogical treasury of words”. Scientist.2001;15:8
- Smelov V, Naber K, Bjerklund Johansen TE. Letter to the Editor: Diagnostic Criteria in Urological Diseases do not Always Match with Findings by Extended Culture techniques and Metagenomic Sequencing of 16S rDNA. The Open Microbiology Journal 2016;10:23-26
- Kass EH. Chemotherapeutic and antibiotic drugs in the management of infections of the urinary tract. Am J Med 1955;18:764-7817
- EAU Guidelines on Urological Infections M. Grabe (Chair), R. Bartoletti, T.E. Bjerklund Johansen, T. Cai (Guidelines Associate), M. Çek, B. Köves (Guidelines Associate), K.G. Naber, R.S. Pickard, P. Tenke, F. Wagenlehner, B. Wullt (http://uroweb.org/guideline/urological-infections/). European Association of Urology, 2015
- Stamm WE, Counts GW, Running KR, Fihn S, Turck M, Holmes KK: Diagnosis of coliform infection in acutely dysuric women. New Engl. J Med 1982;307:463-468
- Bjerklund Johansen TE, Botto H, Cek M et al. Critical review of current definitions of urinary tract infections and proposal of an EAU/ESIU classification system. IJAA 2011;38(Suppl):64-70
- Smelov V, Naber K, Bjerklund Johansen TE. Improved Classification of Urinary Tract Infection: Future Conisderations. Eur Urol Suppl. 2016;15:71-80
- Benson M, Jodal U, Agace W, Andreasson A, Mårild S, Stokland E, et al. Interleukin-6 and interleukin-8 in children with febrile urinary tract infection and asymptomatic bacteriuria. J Infect Dis. 1996;174:1080-4
- Frendeus B, Godaly G, Hang L, Karpman D, Svanborg C. Interleukin-8 receptor deficiency confers susceptibility to acute pyelonephritis. J Infect Dis. 2001;183 Suppl 1:S56-60.
- Ragnarsdottir B, Samuelsson M, Gustafsson MC, Leijonhufvud I, Karpman D, Svanborg C. Reduced toll-like receptor 4 expression in children with asymptomatic bacteriuria. J Infect Dis. 2007;196(3):475-84.
- Mûnger K, Baldwin A, Edwards KM, Hayakawa H, Nguyen CL, Owens M et al. Mechanisms of Human Papillomavirus-Induced Oncogenesis. J Virol 2004; 28 (Nov):11451-11460
- Bardia A, Platz EA, Yegnasubramanian S, demarco AM, Nelson WG. Anti-inflammatory drugs, antioxydants, and prostate cancer. Curr Opin Pharnmacol 2009;9:419-26
- McCarron SI, Edwars SP, Evans PR , Gibbs R, Deamaley DP, Dowe A et al. Influence of cytokine gene polymorphisms on the development of prostate cancer. Cancer res 2002;62:3369-72
- Jounai N, Kobiyama K, Takeshita F, Ken J. Ishii KJ. Recognition of damage-associated molecular patterns related to nucleic acids during inflammation and vaccination. Front Cell Infect Microbiol 2012; 2: 168. doi:10.3389/fcimb.2012.0016818
- Steinhagen F, Kinjo T, Bode C, Klinman DM. TLR-based immune adjuvants. Vaccine 2011;29(17):3341-3355
- Cai T, Mazzoli S, Mondaini N, Meacci F, Nesi G, D’Elia C, Malossini G, Boddi V, Bartoletti R. The roleof asymptomatic bacteriuria in young women with recurrent urinary tract infections: to treat or not to treat? Clinical Infectious Diseases 2012; 55(6):771-7
- Wullt B, Sundén F. Asymptomatic bacteriuria with the model strain Escherichia coli 83972 protects against symptomatic urinary tract infections. In: Naber KG, Schaeffer AJ, Heyns C, Matsumoto T, Shoskes D, Bjerklund- Johansen TE, eds. Urogenital infections. Arnhem, Netherlands: European Association of Urology–International Consultation on Urological Diseases, 2010:314–8
- Boursi B, Mamtani R, Haynes K, Yu-Xiao Yang. Recurrent antibiotic exposure may promote cancer formation – Another step in understanding the role of the human micorbiota? Eur J Cancer 2015;51:2655-2664
Note from editor: This article was previously published in European Urology Today, EAU’s 2017 Congress News.