Eivind Storaas, MD1. Turnuslege, sykehuset i Vestfold, eivisto@gmail.com
Adrian Kinzel. Medical Director Europe, Germany, Novocure
Uri Weinberg . VP of Research & Development, Switzerland, Novocure
Eivind Storaas
ABBREVIATIONS
CNS: central nervous system
FDA: Food and Drug Administration
HR: hazard ratio
ITT: intention to treat
kHz: kilohertz; frequency equivalent to 1000 cycles per second
mITT: modified intention to treat
MRI: magnetic resonance imaging
OS: overall survival
PFS: progression-free survival
PRiDe: Patient Registry Dataset
TMZ: temozolomide
TTFields: tumor treating fields
V/cm: volts per centimeter; unit of intensity measurement of electric fields
VEFG: vascular endothelial growth factor

Introduction
Glioblastomas (also known as glioblastoma multiforme or grade IV astrocytoma) are the most common type of primary malignant brain tumor in adults, and the most deadly.1,2 Approximately 90% develop de novo from normal astrocytes and exhibit rapid growth (primary glioblastomas), while the remainder develop from low-grade astrocytomas and grow more slowly (secondary glioblastomas).2 Glioblastomas are highly vascularized and extremely proliferative invasive tumors with significant genetic and phenotypic heterogeneity.2,3
Population studies indicate an age-adjusted incidence rate for glioblastoma that ranges from 0.59 to 3.69 per 100 000 persons.4 Norway has roughly 200 new glioblastoma diagnoses per year. The incidence of glioblastoma increases with age worldwide, and peaks in individuals aged 75-84 years.6
Despite modest improvements over the past 3 decades, overall survival (OS) for newly diagnosed patients remains a dismal 15 months with the current standard of care of surgical resection followed by concomitant radiation and temozolomide (TMZ) then maintenance TMZ,7-9 with a 5-year survival rate around 5%-10%.6,10,11 Prognosis is particularly poor for those with recurrent disease and the elderly.12 For patients with recurrent glioblastoma, the median progression-free survival (PFS) is 16 weeks (3.7 months) to 18 weeks (4.2 months) and the median OS is 31 weeks (7.1 months) to 40 weeks (9.2 months) with current treatment regimens.13,14 As for elderly patients newly diagnosed with glioblastoma, median OS is only about 4 to 5 months, 12 with a 5-year survival rate of <2% for those aged 65 years or older.6 Often, elderly patients do not receive multimodal therapy, in part due to comorbidities as well as a desire to balance the potential survival benefit associated with more aggressive therapy with the risk of treatment-associated toxicity.12
Proposed obstacles to more effective treatment include the widely infiltrative tumor growth, which typically precludes definitive surgical resection; the general barrier to chemotherapy delivery posed by the blood-brain barrier; intrinsic resistance of glioblastoma cells (with DNA repair enzyme MGMT) to alkylating chemotherapies; toxicity associated with increasing radiotherapy doses; and the difficulties of targeted therapy due to inter- and intra-tumoral heterogeneity.15-17 Recent data using Optune™ (formerly NovoTTF™-100A System; Novocure Ltd., Haifa, Israel), a medical device that utilizes tumor-treating fields or TTFields (also known as alternating electric fields) to treat glioblastoma, has generated exciting results and has redefined the current standard of care for newly diagnosed GBM patients.
The data with this novel treatment strategy for glioblastoma is examined below, following a review of evolving care for glioblastoma.
Evolution of glioblastoma treatment
Early (pre-temozolomide) era
Surgically debulking—to the maximum extent consistent with neurological function—followed by radiotherapy had become an early standard of care for glioblastoma by the early 1990s,18,19 but the role of chemotherapy remained controversial for some time afterwards. Initial chemotherapy for glioblastoma focused on intravenous injection of nitrosoureas, lipid-soluble drugs capable of crossing the blood-brain barrier.17 However, a meta-analysis of nitrosoureas studies revealed only a modest 5% increase in 2-year survival when nitrosoureas were combined with adjuvant radiotherapy.17 In addition, further analyses failed to demonstrate benefit of nitrosoureas in any particular clinical subgroup. As a result, investigators began to explore other potential chemotherapy options. Carmustine polymer wafers remain a currently approved treatment option in both Europe and the United states but have never demonstrated sufficient enough benefit to warrant widespread use. 9,17 TMZ became the chemotherapy of choice for further investigation based on greater penetration of the blood-brain barrier, better bioavailability, and better tolerability than previous alkylating agents.
Temozolomide era
A landmark, 2005 phase 3 study comparing radiotherapy alone with radiotherapy plus concomitant and maintenance TMZ in newly diagnosed glioblastoma patients who had undergone surgery reported a median OS of 14.6 months with TMZ plus radiotherapy versus 12.1 months with radiotherapy alone (hazard ratio [HR], 0.63; P<.001).11 As a result, the standard of care for patients with newly diagnosed glioblastoma became maximal surgical resection followed by concomitant radiotherapy and TMZ, followed by maintenance TMZ.9 A subsequent 5-year analysis showed 2-year and 5-year survival rates of 27.2% and 9.8% with TMZ versus 10.9% and 1.9% with radiotherapy alone.11
In contrast to newly diagnosed glioblastoma, there is no standard of care for patients with recurrent glioblastoma, despite the fact that virtually all patients with glioblastoma relapse.20 Potential treatment options include re-resection, reirradiation, TMZ-rechallenge, radiosurgery, chemotherapy-impregnated wafers (in combination with re-resection), bevacizumab, lomustine (plus bevacizumab), and – most recently – TTFields therapy.20,21 As discussed below, bevacizumab is an antiangiogenic agent that has been approved as treatment for recurrent glioblastoma in the United States – but not Europe.22
Post TMZ Pharmacotherapies: bevacizumab
Bevacizumab is a monoclonal antibody to vascular endothelial growth factor (VEGF) that has been studied in both newly diagnosed and recurrent glioblastoma patients. By binding VEGF, bevacizumab inhibits the angiogenesis that has been associated with glioblastoma.9 In one phase 3 trial of patients with newly diagnosed glioblastoma (RTOG 0825), adding bevacizumab to radiation plus TMZ and then as maintenance therapy with TMZ failed to significantly improve OS or the prespecified improvement target for PFS compared with placebo.9 A second phase 3 trial utilizing a similar treatment strategy (AVAglio) again failed to demonstrate an OS benefit with bevacizumab, although PFS was significantly improved in the bevacizumab versus placebo group.9 Based on these data, bevacizumab is not an approved treatment for newly diagnosed glioblastoma.
By contrast, bevacizumab did receive accelerated approval from the United States Food and Drug Administration (FDA) for the treatment of recurrent glioblastoma based on strong radiographic response rates (28%-35%) and 6-month PFS rates (29%-50%) in two prospective noncomparative phase 2 trials.9 However, the European regulatory authority has not approved bevacizumab for recurrent glioblastoma, citing the lack of a control arm in these two phase 2 trials. Recurrent glioblastomas that progress following bevacizumab are typically resistant to further chemotherapy, with a median OS of only 10 weeks following bevacizumab failure.10
TTFields therapy for glioblastoma
TTFields (Optune, Novocure) is an established antimitotic treatment modality that has been approved for the treatment of glioblastoma in the European Union, Switzerland, Australia, and Israel, receiving a CE mark in 2007. Optune is approved for use in recurrent GBM in Japan and the United States, where data evaluating TTFields therapy as potential treatment for newly diagnosed glioblastoma recently resulted in an expanded indication by the FDA to include these patients.24
Mechanism of action and usage
TTFields have a unique mechanism of action that bypasses the blood-brain barrier to deliver growth-suppressing, and ultimately lethal, electric fields to glioblastoma cells possibly independent of tumoral heterogeneity. Components of Optune are illustrated in Figure 1. The system delivers low-intensity (>0.7 V/cm), intermediate-frequency (200 kHz), alternating electric fields or Tumor Treating Fields (TTFields) to the brain via non-invasive transducer arrays attached to the shaved scalp of glioblastoma patients.

Figur 1. Optune Components. The system consists of a plug in power supply, 4 insulated transducer arrays, an electric field generator (the device), a connection cable and box, a portable battery, a charger for portable batteries, and a carrying case (backpack). The device and battery can be worn with a backpack. Images reprinted with permission from Novocure Ltd.
Optimal placement of transducer arrays is based on MRI data for the patient, allowing for personalized patient planning that maximizes filed intensity to the tumor location. Treatment parameters for glioblastoma are preset at 200 kHz with a minimal field intensity of 0.7 V/cm, requiring no adjustment by physician or patient.27 Recommended use for maximal benefit is at least 18 hours a day (75% of each 24-hour period), as well as continued treatment for at least 4 weeks.28 Data indicate that 15% of patients with recurrent glioblastoma experience slowly developing but durable tumor response with TTFields therapy, and that some responders exhibit initial tumor growth before shrinkage.29-31 Hence, treatment should not be discontinued based solely on early radiographic changes.
Optune represents a treatment modality for glioblastoma that is complementary with chemotherapy after surgery and radiation. Optune selectively kills or arrests the growth of rapidly dividing cancer cells like glioblastoma by disrupting mitotic spindle formation during metaphase-to-anaphase transition and by producing a dielectrophoretic effect during telophase that interferes with organelle and macromolecule segregation within daughter cells.27 Some of the cells that do divide produce unhealthy daughter cells with damaged chromosomes, ultimately leading to apoptosis (Figure 2).32
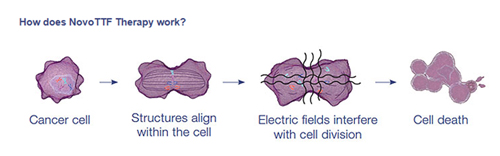
Figur 2. TTFields disrupt mitosis of glioblastoma or other rapidly dividing cells, leading to apoptosis (programmed cell death).
Because TTFields are delivered locally, they do not produce systemic side effects.33,34 The most common adverse effects in glioblastoma patients receiving TTFields therapy have been localized skin reactions or heat sensations of mild to moderate severity. In a study group, there was noted one case of localized skin ulceration.33,34 Systemic adverse events associated with chemotherapy have typically not been observed with TTFields therapy.33,34 The low toxicity of Optune makes it an attractive option for use in combination with chemotherapy for the treatment of glioblastoma.
Treatment of recurrent glioblastoma
Support for TTFields therapy in recurrent glioblastoma was obtained from the phase 3 (EF-11) trial, which compared TTFields therapy with best active chemotherapy by physician’s choice in patients with recurrent glioblastoma.34 Median OS in the intention to treat (ITT) population was 6.6 months for the TTFields group and 6.0 months for best active chemotherapy group (HR, 0.86; P=.27). PFS rates were also similar for the two groups (21.4% and 15.1%; P=.13). On the other hand, the rate of severe adverse events was significantly lower with TTFields therapy, and quality of life measures also favored TTFields therapy over best active chemotherapy. Hence, TTFields therapy was approved for recurrent glioblastoma based on similar efficacy as best active chemotherapy, with better tolerability and higher quality of life.

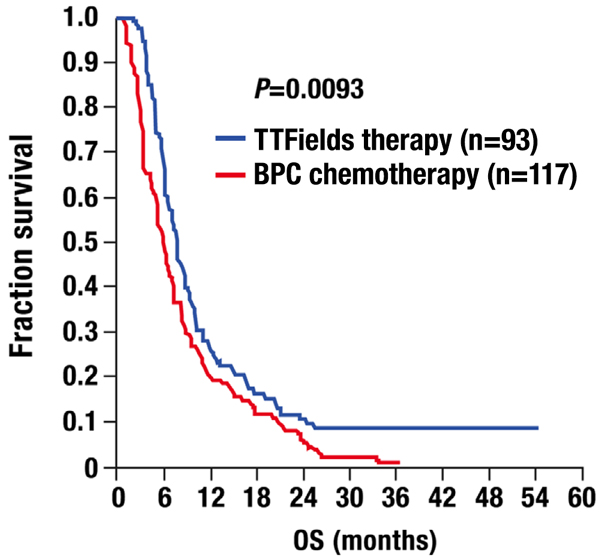
Figur 3. Kaplan-Meier overall survival for the modified intention-to-treat (mITT) population of the pivotal EF-11 trial of TTFields therapy in recurrent glioblastoma. (BPC = best physician’s choice active chemotherapy).
A subsequent post-hoc analysis of the EF-11 OS data focused on the modified ITT (mITT) reported a significantly longer median OS with TTFields therapy versus best active chemotherapy (7.8 vs 6.0 months; HR, 0.69; P=.0093), representing a roughly 30% reduction in risk of death with TTFields therapy (Figure 3).35 This mITT analysis corrected for the 23 patients in the ITT population of the TTFields group who failed to receive at least 1 full treatment course, while all but 1 patient in the ITT population of the active chemotherapy group received at least 1 full treatment course. A full treatment course for TTFields therapy was 28 days, which is consistent with recommended or intended use. The data from this post-hoc analysis suggest that, when used as intended in patients with recurrent glioblastoma, TTFields therapy is associated with superior efficacy compared to the best active chemotherapy, as well as better tolerability and quality of life in the vast majority of patients.
Unlike chemotherapy, TTFields therapy does not have a half-life that lasts beyond administration, and is only effective during time of application. For maximal effectiveness, recommended administration of TTFields therapy is at least 18 hours a day for at least 4 full weeks.28 High daily compliance rates have been associated with longer median OS and increased likelihood of an objective response.31,35 Figure 4 illustrates the results from a recent post-hoc analyses of the EF-11 trial data examining the impact of treatment compliance on median OS.35 As seen, patients receiving TTFields therapy with a maximal compliance rate ≥75% (≥18 hours a day) had a longer median OS than patients with a <75% compliance rate (7.7 versus 4.5 months; P=.042). A significant trend for improved median OS with higher compliance was also observed via Kaplan-Meier analysis.35 Patient compliance also has been shown to be a predictor of tumor response and median OS in additional post-hoc analyses of the EF-11 data (Table 1).
| Tabell 1: Response, median overall survival, and compliance with TTFields therapy in the Phase 3 EF-11 study. (Adapted from Vymazal & Wong, 2014.31) | |||||
|---|---|---|---|---|---|
| Response | Median OS (mo) | Average compliance (average % per 24 h | n | Comparison to responders (PR+CR) | |
| Hazard ratio (95% CI) | Log rank P value | ||||
| PR and CR | 24.7 | 92 | 14 | ||
| SD | 7.6 | 85 | 34 | 0.28 (0.14–0.58) | .0006 |
| PD | 5.5 | 79 | 59 | 0.24 (0.14–0.42) | <.0001 |
| No follow-up MRI (NA) | 2.4 | 60 | 13 | 0.08 (0.02–0.26) | <.0001 |
| All patients | 6.6 | 83 | 120 | ||
| Abbreviations: OS, overall survival; CI, confidence interval; PR, partial response; CR, complete response; SD, stable disease; PD, progressive disease. | |||||
Clinical practice experience from the Patient Registry Dataset (PRiDe), published in 2014, also supports the use of TTFields therapy for patients with recurrent glioblastoma. This study reported the findings for 457 unselected patients with recurrent glioblastoma who received TTFields therapy in a clinical practice setting across 91 cancer centers in the United States between October 2011 and November 2013.33 The most common adverse events associated with TTFields therapy in both settings were mild to moderate skin reactions localized to the scalp beneath the transducer arrays that were easily treated with topical corticosteroids and usually did not require treatment interruption. Median OS for patients in the PRiDe registry compared favorably with the results for the TTFields therapy group (ITT population) in the EF-11 trial (9.6 vs 6.6 months), but some of the difference may have resulted from a higher percentage of patients with first recurrence in PRiDe (33% vs 9%). Particularly impressive median OS was observed in PRiDe when the analysis was restricted to patients who used TTFields therapy as intended (daily compliance ≥75% or ≥18 hours daily) (13.5 months vs 4.0 months for those who had suboptimal compliance).
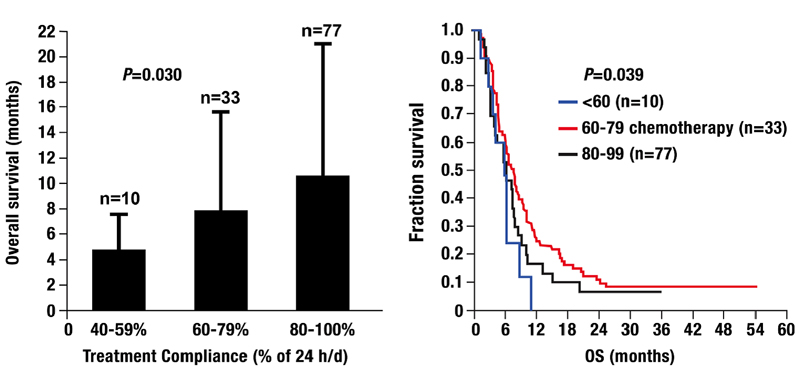
Figur 4. (A) Spearman rank correlation between TTFields therapy compliance and mean overall survival (OS). (B) Kaplan-Meier OS curves stratified according to compliance (<60%, 60%–79%, and 80%–90%).
A comprehensive evaluation of available treatment options should occur for all patients with recurrent glioblastoma. Optune may be an appropriate first choice in suitable patients. A suitable patient should exhibit willingness and capacity to comply with Optune as recommended. As just mentioned, optimal efficacy with Optune has been demonstrated with a daily compliance of ≥75% (≥18 hours daily) for at least 4 weeks duration.33,35 Post-hoc analyses of the EF-11 phase 3 trial data also indicated a significantly higher median OS with Optune in patients with a Karnofsky performance status (KPS) ≥80, tumor size ≥18 cm2, or a prior low-grade.35 Patients with these characteristics may be expected to benefit most from Optune treatment. The PRiDe dataset also highlighted first and second versus third and subsequent recurrences as favorable prognostic factors in Optune-treated patients with recurrent glioblastoma.33 Patients with recurrent glioblastoma and comorbidities may also be well suited for Optune, given the low systemic toxicity associated with this treatment.
Treatment of newly diagnosed glioblastoma
Full data results were presented by Dr. Stupp at the 2015 annual meeting of American Society for Clinical Oncology (ASCO) for a prospective, randomized, multicenter phase 3 trial (EF-14) comparing TTFields therapy plus TMZ with TMZ alone as maintenance therapy in patients with newly diagnosed glioblastoma who had undergone maximal debulking surgery and completed initial treatment with radiotherapy plus adjuvant TMZ.36 The primary study end point was median PFS in the ITT population, and the study was powered for OS as a secondary end point. The prespecified interim analysis was scheduled to be performed on median PFS and median OS data after the first 315 patients had accrued a minimum 18-month follow-up. That data cutoff was achieved in September 2014 and included 210 patients in the TTF-plus-TMZ treatment group and 105 in the TMZ-alone group. The two groups were well matched for age, tumor resection, KPS, and MGMT.
The results of the full analysis demonstrated that the percentage of patients alive at two years when treated with TTFields together with temozolomide was 43% (95% confidence interval 36-50%) compared to 29% (95% confidence interval 21-38%) when treated with temozolomide alone. Patients treated with TTFields together with temozolomide demonstrated a significant increase in progression free survival compared to temozolomide alone (median PFS of 7.1 months compared to 4.2 months, hazard ratio=0.69, P=0.001). Patients treated with TTFields together with temozolomide demonstrated a significant increase in overall survival compared to temozolomide alone (median OS from randomization of 19.4 months compared to 16.6 months, hazard ratio=0.75, P=0.022).36
Based on the results of the initial interim analysis, which was presented at the 2014 Society for Neuro-Oncology (SNO) Annual Meeting, the Data Monitoring Committee recommended early termination of the study due to its overwhelming success. The Committee also recommended that patients in the control (TMZ-alone) arm should be allowed to crossover to the TTFields-plus-TMZ arm prior to disease progression. Dr. Roger Stupp, MD, Director of the University Hospital Cancer Center at the University of Zurich, Zurich, Switzerland, characterized the trial results as “spectacular,” adding, “A new standard of care for patients suffering from glioblastoma is born.”23
Conclusions and summary
Glioblastomas are an extremely deadly form of brain cancer with properties making them difficult to treat with traditional treatment modalities, including surgery, radiation, and chemotherapy. Even with best standard care, the median OS is only 15 months for patients with newly diagnosed glioblastoma, with a 5-year survival rate of around 5%-10%. Moreover, virtually all cases of glioblastoma eventually recur, with an even worse prognosis (few patients with recurrent disease survive more than 3 to 7 months), and few effective treatment options exist. Even recurrent glioblastomas that initially respond to bevacizumab inevitably recur, and these bevacizumab-refractory tumors are particularly resistant to traditional therapies.
Optune represents a unique treatment modality with a novel anti-mitotic mechanism of action and evidence supportive of its use for recurrent glioblastoma and, more recently, newly diagnosed glioblastoma. The recently reported data from EF-14 phase 3 trial and the new US FDA expansion of the indication both point to a new era and new standard of care that includes Optune for patients with newly diagnosed glioblastoma. Optune is currently approved in Europe for the treatment for the treatment of newly diagnosed glioblastoma, after surgery and radiotherapy with adjuvant temozolomide, concomitant to maintenance TMZ.
In addition, Optune is currently approved in the United States for patients with recurrent and newly diagnosed glioblastoma and in the European Union, Switzerland, Australia, Israel, and Japan as monotherapy for recurrent glioblastoma after failure of surgery, radiation, and TMZ.
References
- Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 2007;114:97-109.
- Veliz I, Loo Y, Castillo O, Karachaliou N, Nigro O, Rosell R. Advances and challenges in the molecular biology and treatment of glioblastoma-is there any hope for the future? Ann Transl Med 2015;3:7.
- Urbanska K, Sokolowska J, Szmidt M, Sysa P. Glioblastoma multiforme – an overview. Contemp Oncol (Pozn) 2014;18:307-12.
- Ostrom QT, Bauchet L, Davis FG, et al. The epidemiology of glioma in adults: a ”state of the science” review. Neuro Oncol 2014;16:896-913.
- Cancer Registry of Norway. Cancer in Norway 2011-Cancer incidence, mortality, survival and prevalence in Norway. Oslo: Cancer Registry of Norway, 2013.
- Ostrom QT, Gittleman H, Farah P, et al. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006-2010. Neuro Oncol 2013;15 Suppl 2:ii1-56.
- McNamara MG, Lwin Z, Jiang H, et al. Conditional probability of survival and post-progression survival in patients with glioblastoma in the temozolomide treatment era. J Neurooncol 2014;117:153-60.
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987-96.
- Venur VA, Peereboom DM, Ahluwalia MS. Current medical treatment of glioblastoma. Cancer Treat Res 2015;163:103-15.
- Mehta M, Brem S. Recent updates in the treatment of glioblastoma: introduction. Semin Oncol 2014;41 Suppl 6:S1-3.
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459-66.
- Woehrer A, Bauchet L, Barnholtz-Sloan JS. Glioblastoma survival: has it improved? Evidence from population-based studies. Curr Opin Neurol 2014;27:666-74.
- Friedman HS, Prados MD, Wen PY, et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 2009;27:4733-40.
- Kreisl TN, Kim L, Moore K, et al. Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol 2009;27:740-5.
- Ene CI, Holland EC. Personalized medicine for gliomas. Surg Neurol Int 2015;6:S89-95.
- Huse JT, Holland E, DeAngelis LM. Glioblastoma: molecular analysis and clinical implications. Annu Rev Med 2013;64:59-70.
- Okonogi N, Shirai K, Oike T, et al. Topics in Chemotherapy, Molecular-targeted Therapy, and Immunotherapy for Newly-diagnosed Glioblastoma Multiforme. Anticancer Res 2015;35:1229-35.
- Mornex F, Nayel H, Taillandier L. Radiation therapy for malignant astrocytomas in adults. Radiother Oncol 1993;27:181-92.
- Simpson JR, Horton J, Scott C, et al. Influence of location and extent of surgical resection on survival of patients with glioblastoma multiforme: results of three consecutive Radiation Therapy Oncology Group (RTOG) clinical trials. Int J Radiat Oncol Biol Phys 1993;26:239-44.
- Anton K, Baehring JM, Mayer T. Glioblastoma multiforme: overview of current treatment and future perspectives. Hematol Oncol Clin North Am 2012;26:825-53.
- Taal W, Oosterkamp HM, Walenkamp AM, et al. Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol 2014;15:943-53.
- Avastin [package insert]; South San Francisco, CA: Genentech, Inc.; 2013. Available at http://www.gene.com/download/pdf/avastin_prescribing.pdf.
- Novocure news release. Novocure announces the EF-14 phase III clinical trial of tumor treating fields in patients with newly diagnosed glioblastoma has been terminated at the interim analysis due to early success; November 15, 2014. Available at http://www.novocure.com/news-and-events/news/2014.aspx. Accessed May 12, 2015.
- FDA approves expanded indication for medical device to treat a form of brain cancer. Available at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm465744.htm. Accessed November 24, 2015.
- Novocure news release. Novocure announces Japanese approval of Optune (the NovoTTF-100A System) for treatment of recurrent glioblastoma. March 30, 2015. Available at http://www.novocure.com/news-and-events/news/2015.aspx. Accessed April 1, 2015.
- Novocure Inc. Optune (NovoTTF-100A System). User manual. Issue date: April 2015.
- Lacouture ME, Davis ME, Elzinga G, et al. Characterization and management of dermatologic adverse events with the NovoTTF-100A System, a novel anti-mitotic electric field device for the treatment of recurrent glioblastoma. Semin Oncol 2014;41 Suppl 4:S1-14.
- Novocure Inc. Optune (NovoTTF-100A System). Instructions for use. Issue date: November 2014. Available at http://www.optune.com/resources/educational.aspx. Accessed March 20, 2015.
- Rulseh AM, Keller J, Klener J, et al. Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields. World J Surg Oncol 2012;10:220.
- Villano JL, Williams LE, Watson KS, et al. Delayed response and survival from NovoTTF-100A in recurrent GBM. Med Oncol 2013;30:338.
- Vymazal J, Wong ET. Response patterns of recurrent glioblastomas treated with tumor-treating fields. Semin Oncol 2014;41 Suppl 6:S14-24.
- Benson, L. Technology meets oncology: Understanding the science of tumor treating fields, a novel antimitotic therapy for solid tumors. Poster presented at the Oncology Nursing Society 40th annual congress, April 23-26, 2015.
- Mrugala MM, Engelhard HH, Dinh Tran D, et al. Clinical practice experience with NovoTTF-100A system for glioblastoma: The Patient Registry Dataset (PRiDe). Semin Oncol 2014;41 Suppl 6:S4-S13.
- Stupp R, Wong ET, Kanner AA, et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: a randomised phase III trial of a novel treatment modality. Eur J Cancer 2012;48:2192-202.
- Kanner AA, Wong ET, Villano JL, Ram Z, Investigators EF. Post Hoc analyses of intention-to-treat population in phase III comparison of NovoTTF-100A system versus best physician’s choice chemotherapy. Semin Oncol 2014;41 Suppl 6:S25-34.
- Stupp R, Taillibert S, et al. Tumor treating fields (TTFields): A novel treatment modality added to standard chemo- and radiotherapy in newly diagnosed glioblastoma — First report of the full dataset of the EF14 randomized phase III trial Presented at ASCO 2015; Chicago, IL.