René van Helvoirt. Senior Consultant Oncology, Senter for kreftbehandling / Center for cancer treatment, Sørlandet sykehus, Kristiansand
From the discovery of X rays to the therapeutic use of radiation in lung cancer
Within a year after Wilhelm Conrad Röntgen’s 1895 publication on X-rays, Emil Grubbe reported on using these rays for a recurrent breast tumor. Only five years later, in 1901, Francis Williams was the first to show the curative potential of radiation in cancer treatment when he reported on a patient whose lip cancer disappeared by the treatment. The early Röntgen machines, however, could not generate high enough photon energy levels to penetrate deeper into the body. Therefore, treatment attempts on tumors located deep in the body were not successful. By the late forties, the machine technology had developed so much that photons with megavoltage energy levels could be produced and in 1947, the first publications on radiotherapy in lung cancer emerged. In his concluding remarks on several lung cancer cases, Jackson wrote in 1951 “roentgen therapy has a definite place in the amelioration of symptoms and occasionally unexpected results occur”. Nevertheless, even half a century later, many physicians were still of the opinion that surgery was the only potentially curative treatment available for non-small cell lung cancer (NSCLC) patients. In his 2001 systematic review, Rowell concluded no more than that “radical radiotherapy appears to result in a better survival than might be expected had treatment not been given”. By this time, the published 5-year survival figures of NSCLC patients with locoregionally advanced disease (stage III, table 1), were a disappointing 5 – 15 %.
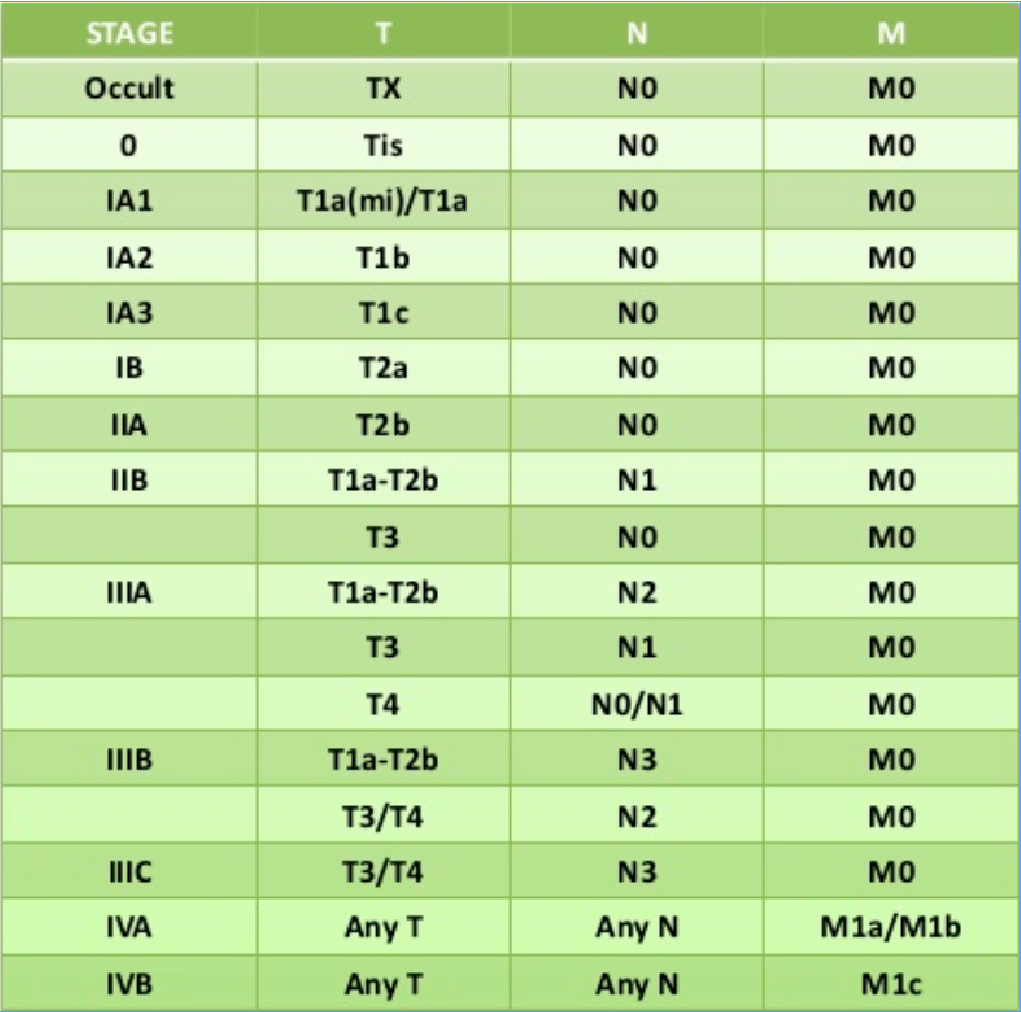
Table 1: 8th Edition of the TNM Classification for Lung Cancer
Advancements in diagnostics, treatment equipment and combined modality treatment
In the past two decades, enormous progress has been made. First, the diagnostic work-up has become much more accurate. With the introduction of PET-CT and MRI scanning and from the development of endo-esophageal / endo-bronchial ultrasound techniques, many fewer patients were wrongly staged and many more patients were properly allocated to a certain treatment protocol. Second, a new generation of linear accelerator radiotherapy machines with adjoining software had come on the market and these allowed for treatments with a higher precision. As result of this higher precision, one was able to escalate the radiation dose to the tumor and/or reduce the dose to the surrounding healthy tissue. Higher tumor doses could lead to better local control (and hopefully better survival) and lower healthy tissue doses would lead to a lower risk of serious side effects. Third, in analogy with other cancer types, successful NSCLC studies were started in which chemotherapy was added to high dose radiotherapy, a combination referred to as chemoradiotherapy. In addition, the very recent Pacific study showed that a further significant overall survival improvement can be obtained by giving immunotherapy after completed chemoradiotherapy in patients with PD-L1 positive tumors (Antonia, 2018; Gray, 2019; see below). So today, there are four possible treatment approaches available for these stage III patients: 1. Surgery (either alone, but often in combination with chemotherapy and/or radiotherapy), 2. Radical radiotherapy alone, 3. Radical chemoradiotherapy (followed by immunotherapy for the PD-L1 positive tumors) and 4. A palliative approach with systemic treatment and/or low- to medium dosed radiotherapy.
Only about 10% of the stage III NSCLC patients will be eligible for surgery. The vast majority is either technically and/or medically inoperable. The percentage of patients considered to be beyond cure, that means the percentage who are allocated to a palliative treatment approach, has been diminishing over the past years. Nowadays, experienced centers offer radical treatment to 65 – 70% of their stage III NSCLC patient population.
From radical radiotherapy only to radical chemoradiotherapy
As chemotherapy had proven its efficacy in other cancer types, for instance in breast cancer, clinical research was started to investigate the role of adding chemotherapy to radical high dosed radiotherapy in stage III NSCLC. One had shown that a cure was possible with high dosed (≥ 60Gy) radiotherapy only, even in stage III. The figures, however, were not positive with a 5-year survival of no more than 4 – 11%. Even in a more recent study, the 5-year survival with radiotherapy did not exceed 10% (Joo, 2015). Several randomized phase III studies from the nineties showed that adding chemotherapy in a sequential way (usually chemotherapy first, radiotherapy thereafter), could double the 5-year survival of these patients, with the best figure now being 23% (e.g. Le Chevalier 1994, Dillman 1996, Sause 2000). The chemotherapy regimens were usually platinum based and doublets, that is platinum combined with another drug (often etoposide or vinorelbine), turned out to be superior over monotherapy.
The next step was made by only changing the time frame of the chemoradiotherapy by giving the chemotherapy concomitantly instead of sequentially. Patients in these studies received two or three platinum-based chemotherapy cycles. Two cycles were given during the 6 – 6,5 weeks of radiotherapy (often 60Gy). A third cycle could be given and if so, this extra cycle was given as an induction treatment 2 – 3 weeks before the start of radiotherapy. Two meta-analyses and a Cochrane report (in total over 2 000 patients) showed without doubt that this concomitant treatment approach is better than the sequential approach. Concomitant treatment leads to a 10% increase in 2-year survival (HR 0,74) and a 4.5% increase in 5-year survival (HR 0,84) (Auperin 2006, Auperin 2010, O’Rourke 2010).
Studies that investigated the possible gain of adjuvant chemotherapy after radiotherapy turned out negative.
From radical chemoradiotherapy to radical chemoradiotherapy combined with immunotherapy
Immunotherapy had proven its palliative efficacy in various stage IV NSCLC patient populations and so the question arose of whether adding immunotherapy in an adjuvant setting would increase the cure rates in stage III disease. This was investigated in the phase III, randomized, double blind, placebo-controlled, multicenter Pacific study. After completed radical platinum-based chemoradiotherapy (with a maximum dose of 66Gy), patients who showed no signs of disease progression were randomized between adjuvant immunotherapy with durvalumab (Imfinzi®) every other week for one year, or placebo treatment. The study showed a significant improvement in both progression free survival and overall survival in the active treatment arm. The median progression free survival was 17.2 months in the durvalumab arm against only 5.6 months in the placebo arm and the latest update reported on a 3-year survival figure of 57% (95% CI 52,3 – 61.4%) for durvalumab against 43.5% (95% CI 37.0 – 49.9%) for placebo (Antonia, 2017; Antonia, 2018; Gray, 2019; figure 1). The toxicity was very acceptable. Patients who were PD-L1 negative did however not benefit from adjuvant durvalumab. Therefore, for PD-L1 positive stage III NSCLC patients who are candidates for radical chemoradiotherapy, adding adjuvant durvalumab is the new standard of care.
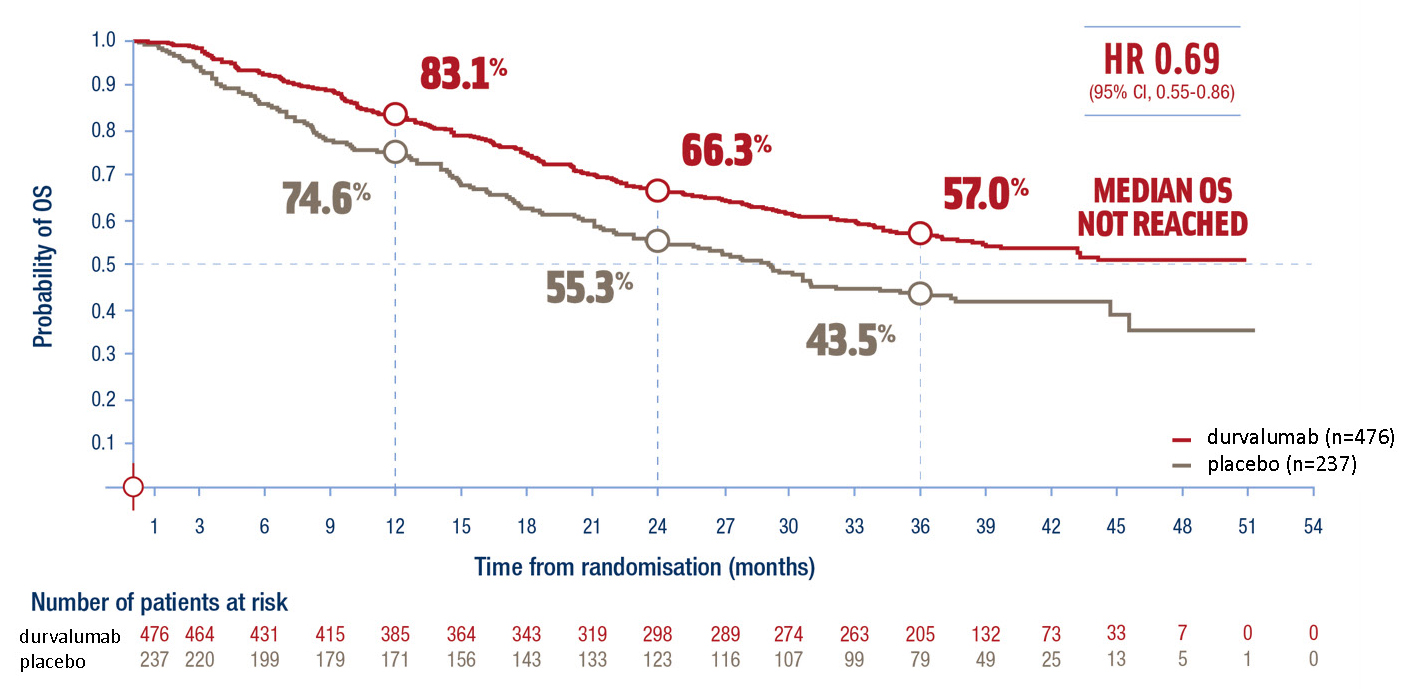
Figure 1: Updated 3-year overall survival from the PACIFIC study, Gray, 2019 (figure supplied by Astra Zeneca)
The optimal dose of radiotherapy
In general, one can assume that higher doses of radiation will lead to more tumor cell kill and thereby to better local control. In addition, if local control is important for survival, better local control will probably lead to better survival. Regarding lung cancer radiotherapy, a multivariate analysis showed that total dose was prognostic for both local control and survival (Willner, 2002). In a phase II study, doses above 69Gy were claimed being optimal for local control and survival (Kong, 2005) and in a randomized phase III study, 68-74Gy turned out being superior over 60-64Gy (Yuan, 2007). Then the RTOG 0617 study was carried out randomizing stage III NSCLC patients to either 60Gy (standard arm) or 74Gy (experimental arm). In the study, the radiation target volume was confined to the primary tumor and the affected lymphatic nodes (so called ‘involved field’ treatment), which means that elective nodal irradiation was not allowed. This is in accordance to all present-day treatment protocols, as previous studies had shown no survival benefit of elective nodal irradiation (elective nodal irradiation means irradiation of clinically and radiologically negative lymphatic nodes that are only assumed to have a certain risk of microscopic tumor spread). To the surprise of many, the study showed a significantly worse survival in the high dosed patients. The median overall survival was 28.7 months for patients who received 60Gy and 20.3 months for patients who received 74Gy (HR 1.38; p=0.004). The 5-year survival was 32.1% in the 60Gy arm, against 23% in the 74Gy arm (HR 1.35) (Bradly, 2015; Bradley, 2017; figure 2). A possible explanation for the worse survival in the high dose arm is treatment related deaths of (cardiac) toxicity. The study has led to a higher focus on the organs at risk in radiotherapy planning and tougher dose constraints, especially for the heart (frequently used constraints are Mean Heart Dose < 20Gy and preferably < 10Gy and V45 < 25%).
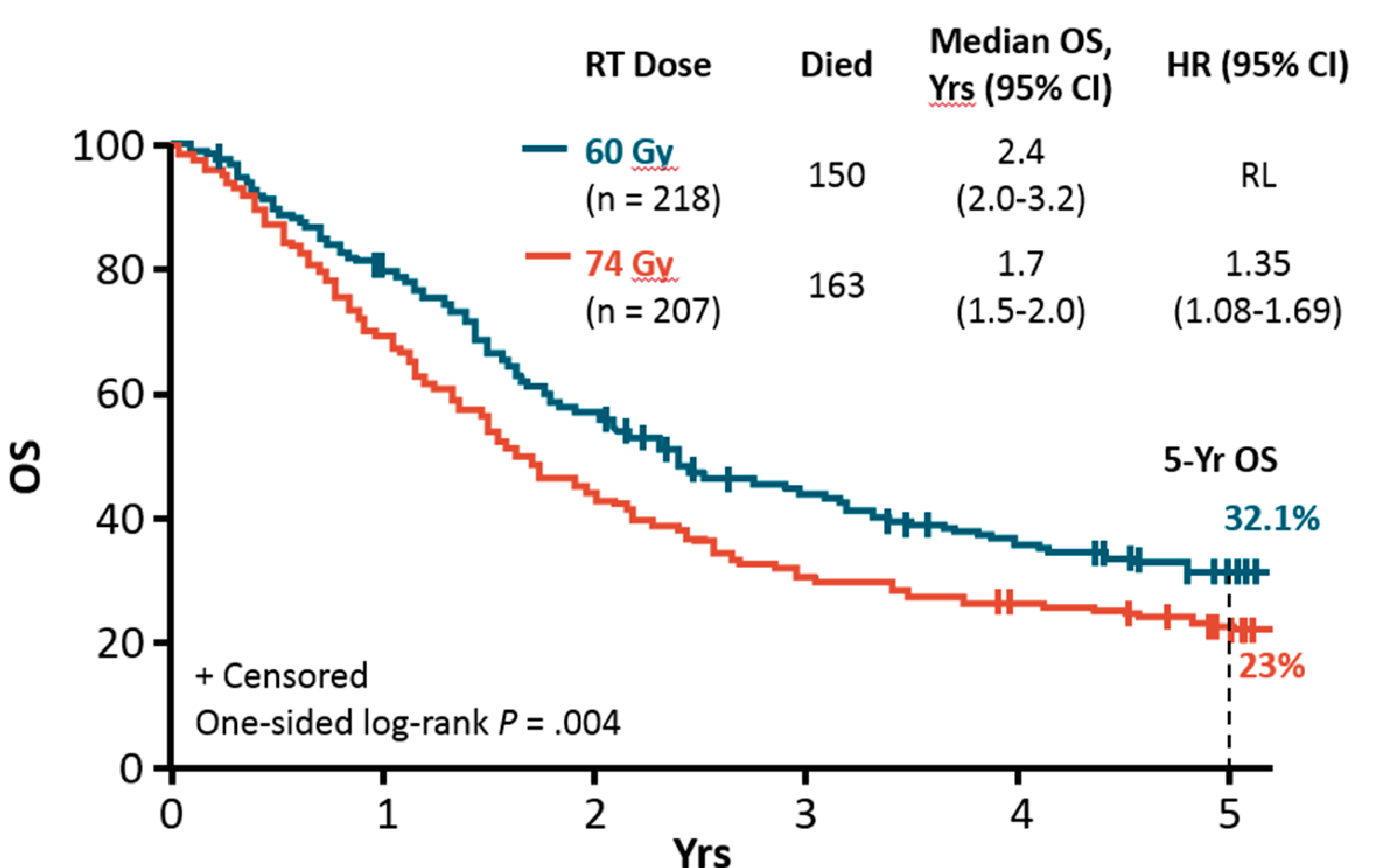
Figure 2: Overall survival RTOG 0617 study, standard dose (60Gy) versus high dose (74Gy)
The question of the optimal radiation dose can still not be answered. If the aim of treatment is curative, the dose should be at least 60Gy. Moderate dose escalation to 66Gy might give a slight survival improvement (Rodrigues, 2015), and many present-day treatment guidelines recommend a dose of 60 – 66Gy.
Even if the RTOG 0617 was a negative study, the 32.1% 5-year survival of the 60Gy standard arm is better than was seen before in other large studies in the stage III NSCLC population. One can conclude that over the past two decades, the optimization of chemoradiotherapy of stage III patients has doubled their 5-year survival chances from below 15% to over 30%. For patients with PD-L1 positive tumors who receive adjuvant immunotherapy with durvalumab, this 5-year figure will hopefully become even better.
Survival in study patients versus survival in everyday patient populations
One would think that the around 30% 5-year survival figures obtained in phase II and III studies would be hard to accomplish in routine everyday practice. Certainly, patients participating in studies are selected and the majority will be of a younger age (< 70), in good performance status, without pathological weight loss and with small to moderate sized tumors. Thereby they do not exactly reflect our everyday patient population. However, several published population-based survival figures are in fact of the same magnitude (e.g. De Ruysscher, 2012).
Patient selection
As shown, radical non-surgical treatment has a curative potential for stage III NSCLC. However patients who are offered palliative treatment, will have a very low probability of being alive 5 years after diagnosis. To put it differently, radical chemoradiotherapy should be the default treatment choice for such patients, and one should come with solid arguments if one decides not to offer this to the patient. Counter arguments have been used, and probably sometimes still are used, are related to large tumor size, N3 nodal disease, high patient age, pathological weight loss and poor performance status. These aspects are discussed successively here.
Large tumor size
Patients having primary tumors with a size of more than 7-8 cm in diameter were sometimes considered ineligible for radical treatment. There is however no solid support for this size argument in the literature. In 2013, the IASLC study group published on 868 patients and showed that only small tumors of 3 cm or less confined a significant benefit in median survival. For tumors between 3 and 5 cm, between 5 and 7 cm and over 7 cm, the survival differences were not significant (Ball, 2013). In addition, the Trans-Tasman group investigated the prognostic effect of tumor size in a group of 509 patients and could not find significant differences (Ball, 2013). Of course, large tumor sizes will necessitate large radiation field sizes (especially if also nodal spread must be covered) and sometimes the radiation dose burden to the organs at risk (lungs, heart) will make a high dose radical treatment impossible. If one is in doubt whether it will be possible, one should make a radiation plan and not conclude yes or no before the plan is optimized, and the dose-volume histograms show the consequences of the planned fractionation regimen.
Advanced N stage
The above-mentioned IASLC report also investigated whether the N stage had much to say for the prognosis of the patient. They could not find significant survival differences between the N0, N1, N2 and N3 patient groups (Ball, 2013). In addition, both in the Trans-Tasman patient population and in a 1274-patient cohort published by Rodrigues in 2014, there were no differences between N1, N2 and N3 (Ball, 2013 and Rodrigues, 2014). This means that also patients with advanced lymphatic node spread are potential candidates for radical treatment. Likewise, as discussed above, the necessary radiation field sizes sometimes will become too large to allow for a 60Gy dose and one has to opt for a lower, palliative dose.
High age
Even if a large part of the randomized studies included patients only up to a certain age, there is no evidence of there being a cut-off age value above which radical treatment no longer would be appropriate. Age has shown to be prognostic, but as a continuous variable.
Pathological weight loss
Pathological weight loss is often defined as an unintended loss of 5% of a patients’ original weight over the past 3 months or a loss of 10% over the past 6 months. Patients with such pathological weight loss usually have a worse treatment outcome. However, as there also are studies in which this was not a significant factor, weight loss in itself should not exclude a patient for radical treatment.
Poor performance status
All studies with a focus on performance status (PS) concluded that the treatment outcome for patients with ECOG PS ≥ 2 was bad (e.g. Dudani, 2018). Therefore, except for patients whose poor PS can be attributed to not directly life limiting comorbidity, patients with PS ≥ 2 will usually not be candidates for radical treatment.
To conclude, radical chemoradiotherapy (+/- immunotherapy) should be offered to inoperable patients who are in an acceptable condition, regardless of primary tumor size, N-stage and age.
Smoking
Research in the past two decades on the consequences of continuous smoking in cancer patients has made it clear that cancer patients who smoke have less benefit of radiotherapy, less effect of chemotherapy, significantly more treatment related side effects and a significantly worse disease specific survival and overall survival (Warren, 2014). In 2008, Rades published clinical data in a lung cancer patient cohort showing far worse local control in patients who smoked during radiotherapy (Rades, 2008; figure 3). The 2-year local control rate in active smokers was 34%, and in patients who did not smoke during radiotherapy, it was 58%. It is hard for patients who smoke to quit and studies have shown that adequate physician-based verbal information alone only makes 1 out of 4 patients quit. With an evidence-based smoking cessation support program, the percentage of quitters will increase and success rates of 50% have been reported. So, in the era of evidence-based medicine, smoking cancer patients who are candidates for cancer treatment and who have a reasonable life expectancy (> I year), should be offered participation in a smoking cessation program as part of their treatment.
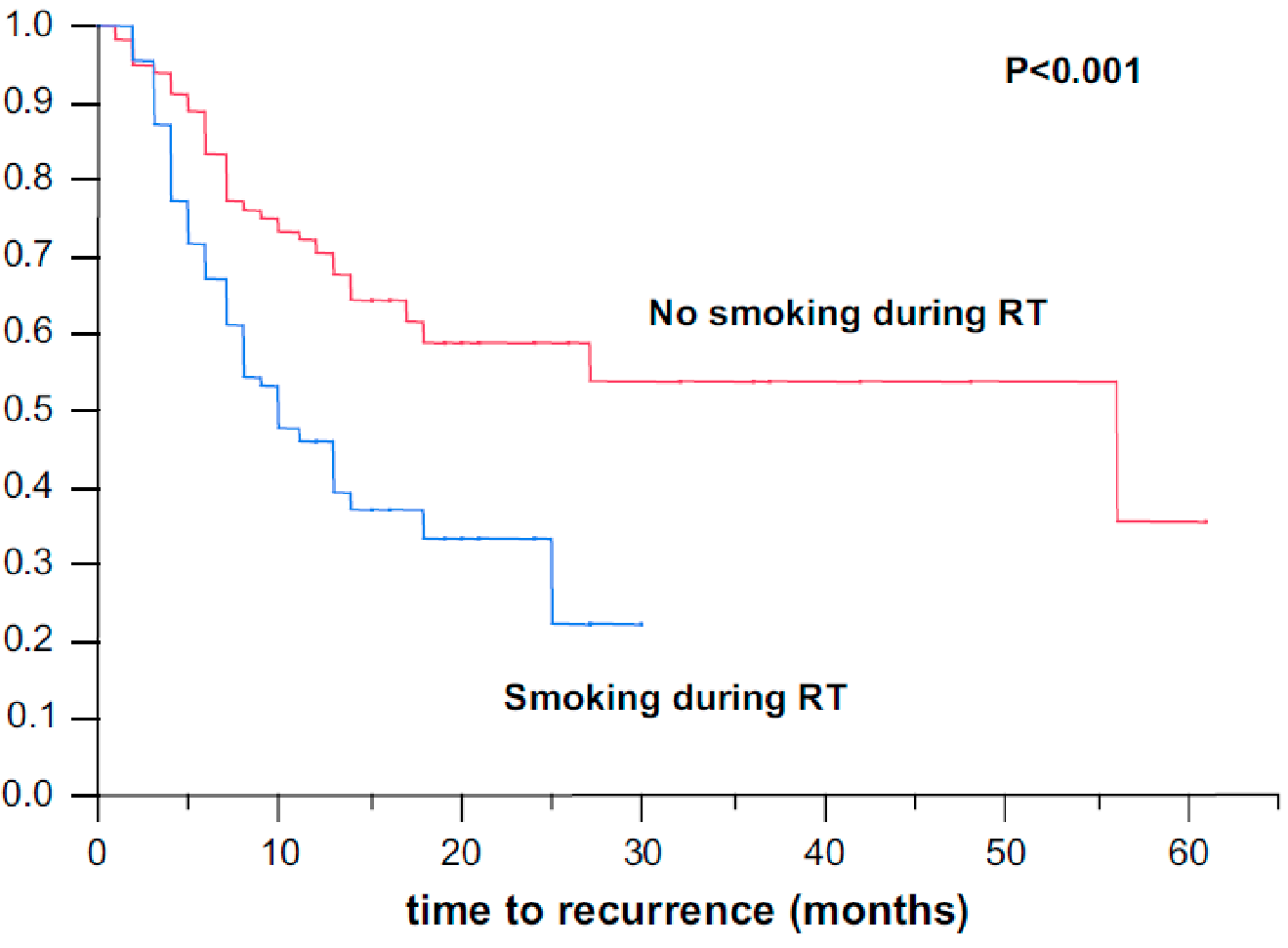
Figure 3: Effect of smoking during radiotherapy (RT) on locoregional control, Rades, 2008
Multidisciplinary team
All (presumed) stage III patients shall have their case discussed in a multidisciplinary team (MDT) setting before the final decision on treatment is made. The members of the thoracic oncology MDT are the radiologist, pulmonologist, thoracic surgeon, clinical oncologist (or medical oncologist + radiation oncologist), and pathologist. In the ideal situation, patients are discussed twice. First briefly at the start when referred to the hospital on the suspicion of lung cancer, just to make decisions on the remaining diagnostic investigations and their sequence. Second, when all the diagnostics are done and the treatment decision is to be made.
For elderly patients with comorbidities, it is strongly recommended to consult a geriatric specialist for an assessment of the patient. Quite a number of these patients have little reserves, even if they look energetic at first sight. Modifications of the planned radical treatment might be necessary (see below). In case of comorbidities that are insufficiently treated, treatment adjustments for these comorbidities might improve the patient’s condition, so that the oncological treatment is better tolerated.
Treatment modifications
As stated above, concomitant platinum based chemoradiotherapy is the treatment of choice. Cisplatin is the preferred drug, as it was used in the majority of studies. But for patients over 75 years of age who are deemed fit enough for the concomitant approach, carboplatin is often a better tolerated alternative. Carboplatin will also be the drug of choice in patients with reduced renal function. In frail patients, the sequential approach with chemotherapy first, followed by radiotherapy, or radiotherapy alone can be chosen. Dose reduced chemotherapy can also be a necessary modification, either already from the start in elderly patients, or for the second (or third) cycle in cases of reduced tolerance (mainly because of bone marrow toxicity).
Moderately dosed chemoradiotherapy as a palliative treatment approach
In case high dose radiotherapy is not possible because of the extent of the disease or because the patient’s lung function is too poor, it is advised not to refrain from radiotherapy, but, if possible, to continue with a palliative chemoradiotherapy approach with a lower dose of radiotherapy. The basis for this recommendation is the phase III Conrad study where patients with advanced stage III disease were randomized between 4 cycles of chemotherapy (carboplatin + vinorelbine) or the same chemotherapy plus 42Gy radiotherapy (fractionation regimen 2,8Gy*15, started parallel or shortly after cycle 2) (Strøm, 2013). Patients who received radiotherapy had a significantly better median progression free survival (7 versus 4.2 months; p<0.001) and overall survival (12.6 versus 9.7 months; p<0.001). After one year, 53.2% of the patients in the chemoradiotherapy arm were alive, against only 34% of the patients in the chemotherapy arm (p<0.01). Furthermore, the health-related quality of life (QoL) was superior in the chemoradiotherapy arm. Following a minor decline during treatment, QoL remained more or less unchanged for the chemoradiotherapy patients, while there was a noteworthy decline for the chemotherapy patients.
Time to treatment start
Proper patient selection and treatment allocation is the cornerstone of treatment, but also time means much. An unnecessary prolongation of the diagnostic work-up time before the start of treatment can worsen the patient’s prognosis significantly. Several studies have shown that there is around a 20% risk of significant tumor progression if the waiting time exceeds 4 weeks (O’Rourke, 2000; Jensen, 2002; Murai, 2012). Knowing this, time frame guidelines have emerged in several countries (e.g. in Norway, table 2). For most of the hospitals, this will only be a matter of logistics. That even simple measures can give a large gain, was shown in a Swedish health region (Holgersson, 2015). They implemented Patient Guides, persons who looked after the patient and steered his or her way through the health system. As a result, the median waiting time from suspicion of lung cancer to the start of treatment in the region, was reduced from 71 to 45 days.
| Lung cancer | Maximum |
|---|---|
| From referral to first hospital appointment | 7 days |
| From first appointment to treatment decision | 21 days |
| From treatment decision to surgery | 14 days |
| From treatment decision to systemic treatment | 7 days |
| From treatment decision to radiotherapy | 14 days |
Side effects
Radical chemoradiotherapy puts an enormous burden on the patient. Besides the well-known side effects of chemotherapy, the patient will suffer from acute, subacute and late side effects of radiotherapy. With regard to the acute side effects, radiation induced esophagitis is the main problem in the majority of patients with T4 and/or N2-3 cancers. The severity of the esophagitis usually exceeds beyond grade 2 and will interfere hugely with food intake and thereby weaken the patient’s general condition. The patient has to be looked after very regularly during the radiation treatment course (e.g. by a nurse) and supportive care is very important. Local anesthetics, pain killers, liquid food supplements and sometimes nasogastric tube feeding are the relevant interventions.
The main problem in the subacute phase, 6-12 weeks after the end of radiotherapy, is radiation pneumonitis. In a portion of the patients this inevitable pneumonitis will be subclinical, in another it will be moderately symptomatic with coughing problems (steroids will then be given) and in a small proportion it can become severely symptomatic with profound dyspnea and necessitate hospitalization and sometimes even respiratory support. Fortunately, with proper patient selection and modern radiotherapy techniques where one confines to the lung dose constraints, the risk of a lethal radiation pneumonitis will be below 2% (Keffer, 2019). The Pacific study did not show a significant increase in the incidence or severity of pneumonitis with durvalumab. The incidence of grade 3/4 pneumonitis was 3.6% in the durvaluamb arm and 3.0% in the placebo arm (Antonia, 2017).
The main late side effects of radiotherapy will be in the lungs, the heart and the esophagus (the latter two of course only if the organ lies within the radiation field). Inevitably, the volume of the lungs that is irradiated to a dose above the tolerance level (18-20Gy) will become afunctional. Lung dose constraints are to be followed to avoid the risk of invalidating or even lethal lung damage (frequently used constraints are Mean Lung Dose ≤ 20Gy, V20 preferably ≤ 35% and V5 preferably ≤ 65%). Radiation-induced cardiovascular disease (RICVD) is a real threat to the heart. Both the coronary arteries, the valves and the myocardium itself are at risk and a high radiation burden leads to both symptomatic cardiac morbidity and an increased mortality risk (Cuomo, 2016). In the esophagus fibrosis and strictures might develop that can give swallowing problems. In case of strictures, blocking or even stenting can be necessary.
Conclusion
Stage III NSCLC patients who are not candidates for surgery must be considered for radical chemoradiotherapy (plus adjuvant immunotherapy in case of PD-L1 positivity) as this treatment offers a realistic chance for cure. With optimal treatment and treatment support, at least 30% of these patients can be alive 5 years after diagnosis.
References
Antonia S.J. et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2017 Nov 16; 377(20):1919-1929
Antonia S.J. et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N Engl J Med. 2018 Dec 13; 379(24):2342-2350.
Auperin, A. et al. Concomitant radio-chemotherapy based on platin compounds in patients with locally advanced non-small cell lung cancer (NSCLC): a meta-analysis of individual data from 1764 patients. Ann Oncol. 2006 Mar; 17(3):473-83.
Auperin A. et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer J Clin Oncol 2010 May 1; 28(13):2181-90.
Ball D. et al. Effect of Tumor Size on Prognosis in Patients Treated with Radical Radiotherapy or Chemoradiotherapy for Non–Small Cell Lung Cancer. J Thorac Oncol. 2013; 8: 315-321)
Ball D. et al. The complex relationship between lung tumor volume and survival in patients with non-small cell lung cancer treated by definitive radiotherapy: A prospective, observational prognostic factor study of the Trans-Tasman Radiation Oncology Group (TROG 99.05). Radiotherapy and Oncology 106 (2013) 305–311.
Bradley J. et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015 Feb; 16(2):187-99
Bradley J. et al. Long-Term Results of RTOG 0617: A Randomized Phase 3 Comparison of Standard Dose versus High Dose Conformal Chemoradiation Therapy +/- Cetuximab for Stage III NSCLC. IJROBP, October 1, 2017, Volume 99, Issue 2, Supplement, Page S105
Cuomo J.R. et al. Novel concepts in radiation-induced cardiovascular disease. World J Cardiol. 2016 Sep 26; 8(9):504-519.
De Ruyssher D. et al. Individualised isotoxic accelerated radiotherapy and chemotherapy are associated with improved long-term survival of patients with stage III NSCLC: a prospective population-based study. Radiother Oncol 2012 Feb; 102(2):228-33.
Dillman R.O. et al. Improved survival in stage III non-small-cell lung cancer: seven-year follow-up of cancer and leukemia group B (CALGB) 8433 trial. Journal of the National Cancer Institute 1996; 88(17): 1210-1215.
Dudani S. et al. Radical Treatment of Stage II None small-cell Lung Cancer with Nonsurgical Approaches: A Multi-institution Report of Outcomes. Clin Lung Cancer. 2018 Jan; 19(1):e11-e18.
Gray J.E. et al. Three-year overall survival with durvalumab after chemoradiotherapy in Stage III NSCLC – Update from PACIFIC, Journal of Thoracic Oncology (2019), doi: https://doi.org/10.1016/j.jtho.2019.10.002.
Holgersson G. et al. Waiting time in lung cancer care. Patient guides provided faster flow. Lakartidningen. 2015 Jun 2; 112.
Jensen A.R. et al. Impact of Delay on Diagnosis and Treatment of Primary Lung Cancer. Acta Oncologica Vol. 41, No. 2, pp. 147–152, 2002
Joo J.H. et al. Definitive radiotherapy alone over 60 Gy for patients unfit for combined treatment to stage II-III non-small cell lung cancer: retrospective analysis. Radiation Oncology (2015) 10:250.
Keffer S. et al. Fatal Radiation Pneumonitis: Literature Review and Case Series. Advances in Rad Oncol. 2019 Aug 31.
Kong F.M. et al. High-dose radiation improved local tumor control and overall survival in patients with inoperable/unresectable non-small-cell lung cancer: long-term results of a radiation dose escalation study. International Journal of Radiation Oncology, Biology, Physics 2005; 63(2): 324-333.
Le Chevalier T. et al. Radiotherapy alone versus combined chemotherapy and radiotherapy in unresectable non-small cell lung carcinoma. Lung Cancer 1994; 10(Suppl 1): S239-S244.
Murai T. et al. Progression of non-small-cell lung cancer during the interval before stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys. 2012 Jan 1; 82(1):463-7.
Sause W. et al. Final results of phase III trial in regionally advanced unresectable non-small cell lung cancer: Radiation Therapy Oncology Group, Eastern Cooperative Oncology Group, and Southwest Oncology Group. Chest 2000; 117(2): 358-64
Strøm H.H. et al. Concurrent palliative chemoradiation leads to survival and quality of life benefits in poor prognosis stage III non-small-cell lung cancer: a randomised trial by the Norwegian Lung Cancer Study Group. British Journal of Cancer (2013) 109, 1467–1475.
Warren G.W. et al. The 2014 Surgeon General’s report: «The health consequences of smoking–50 years of progress»: a paradigm shift in cancer care. Cancer. 2014 Jul 1; 120(13):1914-6. doi: 10.1002/cncr.28695. Epub 2014 Mar 28.
Willner J. et al. Dose, volume, and tumor control prediction in primary radiotherapy of non-small-cell lung cancer. International Journal of Radiation Oncology, Biology, Physics 2002; 52(2): 382-389.
Yuan S. et al. A randomized study of involved-field irradiation versus elective nodal irradiation in combination with concurrent chemotherapy for inoperable stage III nonsmall cell lung cancer. Am J Clin Oncol 2007 Jun; 30(3):239-244.